Limb lengthening is possible and has been performed successfully for over 50 years in Kurgan, Russia. Gavriil A. Ilizarov developed the concept in 1951 after seeing many WWII veterans who had leg fractures that had not healed (nonunions).
 Ilizarov first developed an external fixation frame that was placed around the leg. Knowing that compression of the fracture would help stimulate bone healing, he built a frame that had this capacity. He instructed a patient to gradually compress the nonunion by turning a rod. However, the patient turned the rod the wrong way and caused distraction (separation) of the fracture. Ilizarov noticed that new bone had formed in the gap between the bone ends. This was the beginning of much research and development that showed that limb lengthening was possible, safe and effective.
Ilizarov first developed an external fixation frame that was placed around the leg. Knowing that compression of the fracture would help stimulate bone healing, he built a frame that had this capacity. He instructed a patient to gradually compress the nonunion by turning a rod. However, the patient turned the rod the wrong way and caused distraction (separation) of the fracture. Ilizarov noticed that new bone had formed in the gap between the bone ends. This was the beginning of much research and development that showed that limb lengthening was possible, safe and effective.
Ilizarov and his colleagues performed thousands of limb lengthening procedures in Kurgan, Russia. Russian politics, however, made education and communication with the Western world very difficult. Finally, Italian surgeons started performing and improving the procedure in the early 1980s and a large center soon developed in Lecco, Italy. The first limb lengthening case in the United States was performed in 1988. At first, there was much resistance and skepticism from the US orthopedic community, but limb lengthening has proven to be a very powerful and effective procedure.
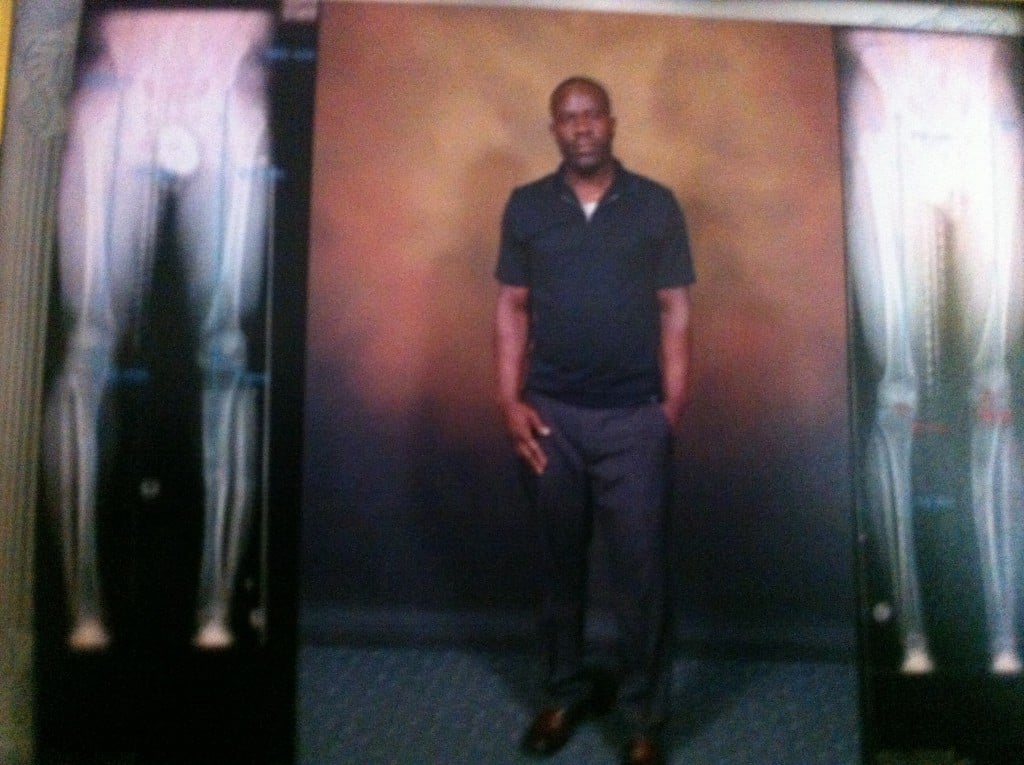
Limb lengthening and reconstruction techniques can be used to replace missing bone and lengthen and/or straighten deformed bone segments. The procedures may be performed on both children and adults who have limb length discrepancies due to birth defects, diseases or injuries. The limb lengthening and deformity correction process works on the principle of distraction osteogenesis. This is a revolutionary concept that reverses the long-held belief that bone cannot be regenerated. In this process, a bone that has been cut during surgery can be gradually distracted (pulled apart), leading to new bone formation (osteogenesis) at the site of the lengthening. In this way, bone segments can be lengthened by 15 to 100 percent of their original length. We use a variety of techniques, including the use of monolateral (one-sided) and circular external fixation devices, to correct angular deformities as well as limb length discrepancies.
We provide opportunities for individuals who previously had no treatment alternatives.
 The regenerated bone is normal and does not wear out. The muscles, nerves and blood vessels grow in response to the slow stretch like they do during a growth spurt or in pregnancy. The actual procedure is minimally invasive and requires only one or two nights in the hospital. Patients aren't in much pain since the distraction is so gradual and patients can continue to walk during the treatment.
The regenerated bone is normal and does not wear out. The muscles, nerves and blood vessels grow in response to the slow stretch like they do during a growth spurt or in pregnancy. The actual procedure is minimally invasive and requires only one or two nights in the hospital. Patients aren't in much pain since the distraction is so gradual and patients can continue to walk during the treatment.
Children and adults can be appropriate candidates for the procedure. Children with congenital deformities such as fibular hemimelia, congenital short femur and hemiatrophy will often have unequal leg length and this may be associated with deformity. Many adults have had this condition since childhood and have developed back pain and hip arthritis from the leg length discrepancy. Growth plate fractures and bone infections in children can cause stunting of growth that results in discrepancy.
Following trauma, bones can heal in a shortened and deformed position (malunion). Sometimes the bone can even remain unhealed (nonunion). Limb lengthening procedures address all of these issues. We have been able to successfully correct large deformities and equalize limbs with discrepancies of several inches. A segment of bone can be missing after a bone tumor, bone infection or severe fracture. We can transport new bone to fill in this defect.
Short stature can be very disabling in patients with dwarfism, for example. We can lengthen both legs simultaneously to increase stature. We have been able to lengthen achondroplastic dwarf patients 12 inches in the legs and five inches in the arms. This allows them to function more independently and be able to reach the telephone, toilet and gas pedal, for example.
Young adult patients with leg deformities are at risk for developing arthritis as a result of their malalignment. These same techniques can be used to correct severe deformities safely and avert the need for joint replacement.
For more information read Dr. Rozbruch's article on Limb Lengthening Surgery.