Hip Replacement
Medically reviewed by William J. Long, MD, FRCSC ; Alexander S. McLawhorn, MD, MBA

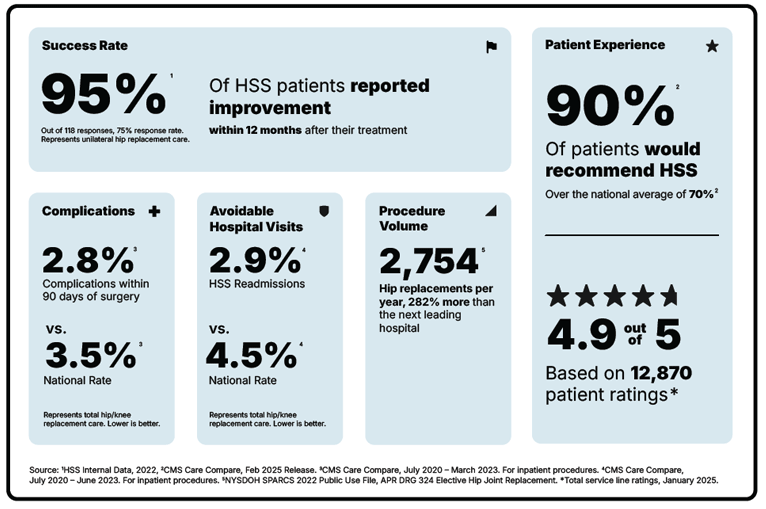
Hip replacement is a highly successful surgery in which portions of the hip joint are replaced with prostheses (implants). Hospital for Special Surgery (HSS) in New York City performs more hip replacements than any other hospital in the United States. It is ranked the #1 hospital for orthopedics in the United States by U.S. News and World Report (2025-2026).
- What is hip replacement surgery?
- How do you know if you need one?
- What are the different types?
- How should I prepare?
- Can it be done as an outpatient?
- How long does the surgery take?
- How long is recovery?
- Can I have both hips done at once?
- What are the risks?
- What are hip implants made of?
- How long do hip implants last?
- When can I resume driving?
- What should I look for in a surgeon?
- How successful is this surgery?
What is hip replacement surgery?
Hip replacement is the removal and replacement of portions of the pelvis and femur (thighbone) that form your hip joint. It is performed primarily to relieve hip pain and stiffness caused by hip arthritis.
This procedure is also sometimes used to treat injuries such as a broken or improperly growing hip, and other degenerative conditions of the hip.
Ask the Expert: Dr. Brian P. Chalmers explains total hip replacement
Brian P. Chalmers, MD, explains how hip replacement surgery works – from why you might need one to how implants work – and why choosing the right specialist matters in getting the best outcome.
An HSS Orthopedic Surgeon Explains Hip Replacement
How do you know if you need a hip replacement?
If you have these arthritis symptoms, you should consider a hip replacement:
- severe hip pain that is not relieved by medication and that interferes with your work, sleep, everyday activity or quality of life
- hip stiffness that restricts motion and makes it difficult to walk or perform other routine activities, such as donning shoes and socks
To learn more, read Here’s What to Know if You Think You Need a Hip Replacement.
Hip anatomy
The hip is a ball-and-socket joint. The ball, located at the top of your femur (thighbone), is called the femoral head. The socket, called the acetabulum, is a part of your pelvis. The ball moves in the socket, allowing your leg to rotate and move forward, backward and sideways.
In a healthy hip, cartilage covers the ball and the socket to help them glide together smoothly. If this cartilage gets worn down or damaged, the bones scrape together and become rough. This condition, osteoarthritis, causes pain and restricts motion. An arthritic hip can make it painful to walk or even to get in or out of a chair. If you have been diagnosed with hip arthritis, you may not need surgery. Nonsteroidal anti-inflammatory drugs (NSAIDs) and/or physical therapy may provide relief. But, if these efforts do not relieve symptoms, you should consult an orthopedic surgeon.
What are the different types of hip replacement surgery?
Total hip replacement is the most common and successful type, although there are two different surgical approaches (for example, posterior and anterior). Hip resurfacing is another type of hip replacement that might be appropriate in some patients. In rare circumstances, a procedure known as hemiarthroplasty or partial hip replacement may be used, typically in the setting of specific types of hip fractures.
Healthy hip
Arthritic hip
Replaced hip

X-ray of a total hip replacement showing the ball, socket and stem implants
Types of hip replacement surgery: Surgical approaches
Although there are many described surgical approaches to the hip, the two most common surgical approach methods for performing a total hip replacement are:
- the posterior approach
- the anterior approach (sometimes called the "mini-anterior approach" or "muscle-sparing hip replacement")
To begin the operation, the hip replacement surgeon will make an incision on either the back (posterior) or front (anterior) of the hip. Both approaches offer pain relief and improvement in walking and movement within weeks of surgery with comparable, low complication rates.
In some instances, the orthopedic surgeon may choose to employ robotic technologies during the surgery.
Total hip replacement animation: Posterior approach
How should I prepare for hip replacement surgery?
There are certain steps patients can take both before and after surgery to improve recovery time and results. It is important to follow the instructions and guidance provided by your orthopedic surgeon, medical team and rehabilitation therapist. Visit Preparing for Your Surgery to get information on preoperative hip replacement classes and patient education materials about joint replacement surgery.
Can hip replacement be done as an outpatient?
Yes, most healthy patients can be dismissed home on the day of surgery. If the anesthesia, medical, or physical therapy teams feel that it is not appropriate to send a patient home, then patients can stay in hospital as long as needed to be cleared for dismissal, which is typically 1 to 2 days. Learn more about same-day hip replacement by reading Outpatient Hip Replacement Surgery: Frequently Asked Questions.
How long does hip replacement surgery take?
Total hip replacement surgery takes about one and a half hours. With setup time and anesthesia time, patients are in the operating room for about two hours. Most patients are eligible to leave the hospital the same day as surgery.
What is the recovery time for a hip replacement?
Your rehabilitation will begin within 24 hours after surgery. Most hip replacement patients progress to walking with a cane, walker or crutches within a day or two after surgery. As the days progress, you will increase the distance and frequency of walking. Full recovery generally takes anywhere from 2 to 8 weeks, depending on the patient's general health and other factors.
If you have total hip replacement surgery at HSS:
- Your recovery will begin immediately following surgery in the Post-Anesthesia Care Unit (PACU), where your medical team will manage your pain and monitor your vital signs.
- Appropriate candidates for outpatient surgery will be discharged on the day of surgery, when medically appropriate.
- Most incisions are closed with dissolvable stitches and glue.
- You will most likely have a waterproof dressing that allows you to shower the day after surgery. The dressing is removed a week after surgery, and the incision is left open to the air.
- The pain management team will assess your medication and use a multifaceted approach to ensure comfort and mobility during the rehabilitation process.
- Within hours of surgery, you will be seen and evaluated by our physical therapy team. Your therapist will help you sit up, get in and out of bed, and practice walking and climbing stairs using a walker, cane or sometimes crutches in preparation for your dismissal home.
Learn more in our series of articles about hip replacement recovery.
Can I have both hips replaced at the same time?
Yes, healthy patients younger than 75 years old who have no history of cardiopulmonary disease may be able to have both hips replaced at once. In some cases, however, it may be better to stage the surgeries.
What are the risks in hip replacement surgery?
Total hip replacement is a major surgery. It is very safe, but every surgery has risks. Possible risks during surgery include blood loss, injury to a nerve or blood vessel, and fracture of either the pelvis or thighbone. Risks shortly after surgery include blood clots in the leg or pelvis, dislocation of the prosthesis, or infection at the surgical site. You should ask your surgeon what the surgical infection rate is for hip replacements at the hospital or facility where you will have your surgery.
HSS has one of the lowest rates of infection for hip replacement surgery. New York State Department of Health reports from 2008-2019 consistently show that HSS had lower infection rates for hip replacement surgeries than the New York State average. Further, the number of infections is also consistently lower than predicted for similar patients across New York state.
Possible longer-term complications after surgery can include hip fracture, dislocation, stiffness or pain, a failure of ingrowth between the bone and implants, or prosthetic infection.is for hip replacements at the hospital or facility where you will have your surgery.
What are hip implants made of?
There are three separate implants: the stem, the ball and the socket.
- The stem, made of metal (usually titanium, cobalt-chrome or stainless steel) is inserted into your natural thighbone. For patients with poor bone quality (osteoporosis), the surgeon may elect to use bone cement to fix the stem to the bone. Otherwise, the bone of the femur grows onto the metal stem, when bone cement is not used.
- The ball is usually made of cobalt-chrome or ceramic and fits on top of the stem.
- The socket is usually a combination of a plastic liner and a porous titanium shell. The pelvic bone grows onto the titanium implant. Sometimes the surgeon elects to use screws through the titanium shell to further secure the implant to the pelvic bone.
Will my new hip set off the metal detector at the airport?
Today's sensitive screening machines will detect the implant but can also effectively identify it. The machine operator will know that it is an implant rather than an unauthorized metal object contained outside the body.
It is still helpful to tell airport security that you have had a hip replacement before entering the screening machine.
How long does a hip replacement last?
In modern-ceramic-on-polyethylene implants – where the ball is made of ceramic and the socket is lined with polyethylene plastic – there is no significant wear even after 20 years, and most of these will last for a person’s lifetime. When a hip implant does need to be replaced because it has loosened or worn out over time, this requires what is called hip revision surgery. At a population level, the lifetime risk of revision hip replacement is less than 5%.
How soon after surgery can I resume driving?
The typical timeframe is 2 to 4 weeks, but the ability to drive is determined by several factors: Patients have to have ceased taking narcotic pain medications and must be able to aggressively move from the gas to the brake. Therefore, returning to driving is usually faster for left sided hip replacement (about two weeks) than right sided hip replacement (about four weeks).
What should I look for in a hip replacement surgeon?
When looking for an orthopedic surgeon to perform your hip replacement surgeon, it’s important to do your research and check the surgeon’s credentials, experience and reputation. It is also important to research the hospital or facility where you will have your operation.
How successful is total hip replacement surgery?
In general, the success rate for hip replacement surgery is high: About 95% of patients experience relief from hip pain. In one study, HSS interviewed patients to learn about their progress. Two years after their surgeries, 99.4% of patients said they had relief from pain, 98.8% said their ability to move was improved, and 97.8% said their quality of life was better because of their surgery.
In rare instances, implant wear, loosening, infection, fracture or dislocation may require revision to a new hip replacement.
Key takeaways
- Hip replacement involves replacing the damaged portions of the hip joint with prosthetic implants to relieve pain and restore mobility.
- The surgery is most often performed to treat severe arthritis but can also address fractures and other degenerative hip conditions.
- Peoples with persistent hip pain, stiffness, or loss of function that does not improve with medication or physical therapy may be candidates for surgery.
- Recovery begins within 24 hours of surgery. Most patients walk with assistance after one or two days and recover fully within 2 to 8 weeks.
- Same-day outpatient hip replacement is an option for many healthy patients,.
- Modern hip implants are highly durable, with many lasting a lifetime.
- More than 95% of hip replacement patients experience major relief from pain, improved movement, and better quality of life.
Why should you choose HSS for hip replacement?
Hip replacement is a surgery focused on reducing pain and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding these data points will help you make the best decision for your care: See hospital reliability data
Explore Related Patient Stories
View All Patient Stories
Cindi Klar
Bronxville, NY
Shoulder Replacement Surgery

Larry Thau
Flemington, NJ
Hip Replacement

Marilyn Murphy
Middle Village, NY
Hip Replacement
Richard Markx
Novato, CA
Hip Replacement

Jane Maldonado
Norwalk, CT
Hip Replacement

Regina Daley
Brooklyn, NY
Hip Replacement
Lynne Calman
New York, NY
Scoliosis
Justin Blasich
Stewart Manor, NY
Hip Replacement

Gail Morton
Highland Lakes, NJ
Hip Replacement
Diana Abreu
Long Valley, NJ
Hip Replacement

Analisa Barrett
Brooklyn, NY
Hip Replacement

Kristen Houser
Glen Gardner, NJ
Hip Replacement
Karen Morgan
Freehold, NJ
Hip Replacement

Gloria Valdez
Bayside, NY
Hip Replacement

Patricia VanDenburg
Leeds, NY
Hip Replacement
Thomas Ferris
Saint James, NC
Hip Replacement

Sonja Browne
Brooklyn, NY
Hip Replacement

Ilene Weiss
Congers, NY
Hip Replacement

Robyn Henning
Nutley, NJ
Hip Replacement

Alan Dumain
Richmond Hill, NY
Hip Replacement
References
- Ackerman IN, Busija L, Lorimer M, de Steiger R, Graves SE. Lifetime Risk of Revision Hip Replacement Surgery in Australia Remains Low: A Population-Level Analysis Using National Registry Data. J Bone Joint Surg Am. 2021 Mar 3;103(5):389-396. doi: 10.2106/JBJS.20.01235. PMID: 33439609. https://pubmed.ncbi.nlm.nih.gov/33439609/
- Bendich I, Landy DC, Do H, Krell E, Diane A, Boettner F, Rodriguez J, Alexiades M, González Della Valle A. Intraoperative Complications and Early Return to the Operating Room in Total Hip Arthroplasty Performed Through the Direct Anterior and Posterior Approaches. An Institutional Experience of Surgeons After Their Learning Curve. J Arthroplasty. 2021 Aug;36(8):2829-2835. doi: 10.1016/j.arth.2021.03.046. Epub 2021 Mar 26. PMID: 33865647. https://pubmed.ncbi.nlm.nih.gov/33865647/
- Bendich I, Vigdorchik JM, Sharma AK, Mayman DJ, Sculco PK, Anderson C, Della Valle AG, Su EP, Jerabek SA. Robotic Assistance for Posterior Approach Total Hip Arthroplasty Is Associated With Lower Risk of Revision for Dislocation When Compared to Manual Techniques. J Arthroplasty. 2022 Jun;37(6):1124-1129. doi: 10.1016/j.arth.2022.01.085. Epub 2022 Feb 4. PMID: 35124193. https://pubmed.ncbi.nlm.nih.gov/35124193/
- Evans JT, Evans JP, Walker RW, Blom AW, Whitehouse MR, Sayers A. How long does a hip replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet. 2019 Feb 16;393(10172):647-654. doi: 10.1016/S0140-6736(18)31665-9. Epub 2019 Feb 14. PMID: 30782340; PMCID: PMC6376618. https://pubmed.ncbi.nlm.nih.gov/30782340/
- González Della Valle A, Sharrock N, Barlow M, Caceres L, Go G, Salvati EA. The modern, hybrid total hip arthroplasty for primary osteoarthritis at the Hospital for Special Surgery. Bone Joint J. 2016 Jan;98-B(1 Suppl A):54-9. doi: 10.1302/0301-620X.98B1.36409. PMID: 26733642. https://pubmed.ncbi.nlm.nih.gov/26733642/
- Koltsov JCB, Marx RG, Bachner E, McLawhorn AS, Lyman S. Risk-Based Hospital and Surgeon-Volume Categories for Total Hip Arthroplasty. J Bone Joint Surg Am. 2018;100(14):1203-1208. doi:10.2106/JBJS.17.00967. https://pubmed.ncbi.nlm.nih.gov/30020125/
- Memtsoudis SG, Cozowicz C, Bekeris J, Bekere D, Liu J, Soffin EM, Mariano ER, Johnson RL, Go G, Hargett MJ, Lee BH, Wendel P, Brouillette M, Kim SJ, Baaklini L, Wetmore DS, Hong G, Goto R, Jivanelli B, Athanassoglou V, Argyra E, Barrington MJ, Borgeat A, De Andres J, El-Boghdadly K, Elkassabany NM, Gautier P, Gerner P, González Della Valle A, Goytizolo E, Guo Z, Hogg R, Kehlet H, Kessler P, Kopp S, Lavand'homme P, Macfarlane A, MacLean C, Mantilla C, McIsaac D, McLawhorn AS, Neal JM, Parks M, Parvizi J, Peng P, Pichler L, Poeran J, Poultsides L, Schwenk ES, Sites BD, Stundner O, Sun EC, Viscusi E, Votta-Velis EG, Wu CL, YaDeau J, Sharrock NE. Peripheral nerve block anesthesia/analgesia for patients undergoing primary hip and knee arthroplasty: recommendations from the International Consensus on Anesthesia-Related Outcomes after Surgery (ICAROS) group based on a systematic review and meta-analysis of current literature. Reg Anesth Pain Med. 2021 Nov;46(11):971-985. doi: 10.1136/rapm-2021-102750. Epub 2021 Aug 25. PMID: 34433647. https://pubmed.ncbi.nlm.nih.gov/34433647/
- Ponzio DY, Poultsides LA, Salvatore A, Lee YY, Memtsoudis SG, Alexiades MM. In-Hospital Morbidity and Postoperative Revisions After Direct Anterior vs Posterior Total Hip Arthroplasty. J Arthroplasty. 2018 May;33(5):1421-1425.e1. doi: 10.1016/j.arth.2017.11.053. Epub 2017 Dec 9. PMID: 29307677. https://pubmed.ncbi.nlm.nih.gov/29307677/
- Vasireddi N, Chandi SK, Neitzke CC, Cororaton AD, Vigdorchik JM, Blevins JL, McLawhorn AS, Gausden EB. Does Approach Matter in Robotic-Assisted Total Hip Arthroplasty? A Comparison of Early Reoperations Between Direct Anterior and Postero-Lateral Approach. J Arthroplasty. 2024 Jul;39(7):1765-1770. doi: 10.1016/j.arth.2024.01.035. Epub 2024 Jan 30. PMID: 38301980. https://pubmed.ncbi.nlm.nih.gov/38301980/
- Hospital-Acquired Infections in New York State, 2019. New York State Department of Health, Albany, NY. October 2021. https://www.health.ny.gov/statistics/facilities/hospital/hospital_acquired_infections/2019/docs/hospital_acquired_infection_p1.pdf. Accessed July 8, 2024.
- Hospital-Acquired Infection (HAI) Rates in New York State Hospitals https://www.health.ny.gov/statistics/facilities/hospital/hospital_acquired_infections/. Accessed July 8, 2024.
- HSS Arthroplasty Registry, 2007-2024. https://www.clinicaltrials.gov/ct2/show/NCT00454506, updated 024-04-08. Accessed July 8, 2024.
- Newsweek's "World's Best Specialized Hospitals 2022." Accessed July 8, 2024.
- U.S. News & World Report "Best Hospitals for Orthopedics." Accessed July 8, 2024.