Osteoporosis
Medically reviewed by Alana C. Serota, MD, CCFP, CCD
Summary: Osteoporosis is a condition that weakens bones and increases fracture risk. It causes no pain or symptoms until a person breaks a bone. It is a leading cause of hip fractures in older people but affects people of all ages, including children. This article explains risk factors, diagnosis, treatment, prevention, and the importance of optimizing bone health around the time of orthopedic surgery to reduce complications.

What is osteoporosis?
Osteoporosis is a condition of low bone quantity and/or poor bone quality. It means that the bones are fragile and prone to fractures. Osteoporosis is a “silent disease,” since there are no warning signs or symptoms until bone fractures occur. In the United States alone, an estimated 1.5 million bone fractures each year are attributed to low bone density.
Who gets osteoporosis?
Osteoporosis and osteopenia can affect people of all ages but become more likely as we age. Women, especially post-menopausal women, have the greatest risk, accounting for about 80% of all cases. A rare but severe form of the disease known as pregnancy and lactation-associated osteoporosis (PLO) affects younger women, usually in the third trimester of pregnancy or during lactation. In these cases, women may develop one or more vertebral fractures of the spine.
Osteoporosis vs. osteoarthritis
Osteoporosis and osteoarthritis are separate conditions with different pathologies, symptoms and treatments.
Ask the Expert: Dr. Linda A. Russell Explains Osteoporosis vs. Osteoarthritis
Learn the key differences between these two common conditions and what they mean for your bone and joint health. HSS Rheumatologist Linda A. Russell, MD, has extensive expertise in osteoporosis and metabolic bone disease, helping patients maintain strength, mobility, and overall health.

An HSS Rheumatologist Explains Osteoporosis versus Osteoarthritis
What are the risk factors for osteoporosis?
Women get osteoporosis more often than do men, and people of Northern and Western European or Asian descent at higher risk than those of other ethnicities.
Other risk factors include:
- Advancing age.
- Family history of osteoporosis.
- Hormonal changes such as low estrogen states in women (for example, post-menopause) and low testosterone states in men.
- Lifestyle factors, including:
- Smoking.
- Consuming excess alcohol.
- Poor nutrition (especially calcium and vitamin D deficiencies).
- The use of certain medications such as corticosteroids.
In addition, people of low weight (less than 127 lbs/57kg) or who have endocrine disorders (such as hyperparathyroidism or hyperthyroidism) or inflammatory disorders are prone to developing osteoporosis.
What are common osteoporosis symptoms?
Osteoporosis is clinically silent – the "silent thief" as doctors call it. The first "symptom" is a broken bone (fracture). However, 2/3 to 3/4 of vertebral fractures of the spine are clinically silent (causing no pain or mobility symptoms) – the silent crime of the silent thief. This is the reason healthcare providers regularly check a person’s height over time and image the entire spine if height loss is detected. Without proactive screening for at-risk patients, osteoporosis will go undetected until a fracture occurs.
Avoiding complications during orthopedic surgery
One study by HSS spine surgeons found that a high number of their lumbar spine surgery patients had previously undiagnosed osteoporosis, highlighting the need for orthopedic surgeons to be watchful for metabolic bone disease in their patients. Perioperative bone health optimization lowers the rate of complications during or after surgery.
What are the complications of osteoporosis?
Complications include loss of height, spinal deformity such as degenerative scoliosis, pain and dysfunction as a result of fractures and/or the surgery needed to repair same. Spinal fractures can lead to kyphosis, and severe kyphosis can cause organ dysfunction (lung capacity restriction, digestive issues) and make people more prone to falls due to their altered center of gravity from being bent over.
Osteoporosis increases the risk of hip fractures, which have a higher risk of mortality (death) from complications than does a myocardial infarction (heart attack)
Animation on osteoporosis of the spine
What causes osteoporosis?
Low bone density in adolescence and early adulthood can be a result of a failure to attain peak bone mineral density. Accelerated bone loss may be particularly noted around menopause and in later years. Many factors, including diet (for example, insufficient levels of calcium and vitamin D intake) and the lack of proper exercise, contribute to low bone density during these periods.
It may also be the result of numerous underlying conditions, many of which are often not readily apparent during a typical doctor visit. Laboratory testing, including blood and urine studies, is helpful in determining possible secondary and contributing causes.
How do you prevent osteoporosis?
Many studies have shown that calcium and vitamin D are essential for bone health. The amount of calcium that individuals need varies, but adults typically require about 1,200 to 1,500 milligrams daily. It is especially important that growing adolescents get adequate calcium in their diets, in order to prevent osteoporosis later in age.
Every day, approximately 10,000 milligrams of calcium move in and out of the skeleton to renew and repair the bone. Food remains the best source of calcium, but some people may need to get additional calcium by taking supplements.
Also crucial for good bone health are:
- Exercise – weightbearing and resistance exercises help build bone and maintain healthy bone.
- Fall prevention – good balance and removing potential dangers around the house.
- Maintaining a healthy weight.
- Quitting or avoiding smoking tobacco.
- Limiting alcohol intake – two or more drinks a day increases the risk of fracture.
How is osteoporosis diagnosed?
A dual-energy X-ray absorptiometry (DXA or "DEXA") bone mineral density test will help your doctor determine whether or not you have osteoporosis. In addition, a blood and urine test will rule out underlying conditions and medical concerns.
How is osteoporosis treated?
Along with continuing the lifestyle involved in preventing osteoporosis such as healthy eating, calcium and vitamin D supplements and limiting risky behavior, your doctor might suggest special medications to increase bone mineral density. The most important goal is to lower risk of fracture. If needed, your doctor will explain the risks and benefits of the various medications offered and work with you on deciding what's best.
For more information, contact the Osteoporosis and Metabolic Bone Health Center at HSS, which was founded to help prevent and treat osteoporosis, and explore the articles below.
Can osteoporosis be reversed?
We now have osteo-anabolic (bone-growing) agents that improve bone density tremendously, in addition to the more traditional anti-resorptive agents that maintain bone density and prevent fractures. Osteoporosis is not yet curable, but our treatments are robustly effective.
Explore Related Patient Stories
View All Patient Stories
Robert Holden
New York, NY
Lupus
Lynne Calman
New York, NY
Scoliosis

Carol Kenney
New York, NY
Osteoporosis

Janet Otto
New York, NY
Osteoporosis

Silvia Juarez-Marazzo
New York, NY
Broken Wrist (Wrist Fracture)

Chany Marcus
New York, NY
Osteoporosis

Maureen Maby
Great Neck, NY
Arm and Elbow Fractures

Abigail Stellpflug
Brooklyn, NY
Broken Hip (Hip Fracture)

James Cobo
Bronx, NY
Osteoporosis

Laura R.
Massapequa, NY
Degenerative Disc Disease

Louis Cieselski
Brooklyn, NY
Spinal Fracture

Helen D’Errico
Miller Place, NY
Scoliosis

Victor Jimenez
Kissimmee, FL
Osteoporosis
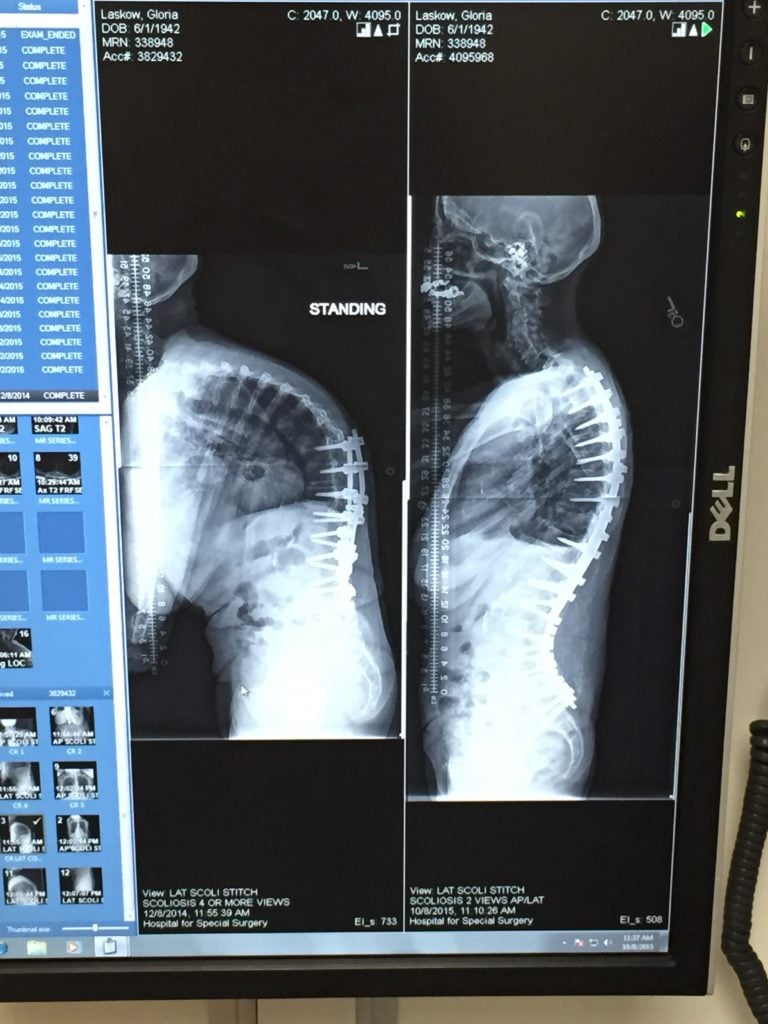
Gloria Laskow
North Babylon, NY
Scoliosis

Michael Simon
New York, NY
Herniated Disc (Bulging Disc)

Connie McKnight
West Hempstead, NY
Osteoporosis

Celine Stahl
Greenwich, CT
Hip Replacement
References
- Cohen A, Kamanda-Kosseh M, Dempster DW, Zhou H, Müller R, Goff E, Colon I, Bucovsky M, Stubby J, Nickolas TL, Stein EM, Recker RR, Lappe JM, Shane E. Women With Pregnancy and Lactation-Associated Osteoporosis (PLO) Have Low Bone Remodeling Rates at the Tissue Level. J Bone Miner Res. 2019;34(9):1552-1561. doi:10.1002/jbmr.3750. https://pubmed.ncbi.nlm.nih.gov/31348548/
- Goolsby MA, Boniquit N. Bone Health in Athletes. Sports Health. 2017 Mar/Apr;9(2):108-117. doi: 10.1177/1941738116677732. Epub 2016 Nov 30. PMID: 27821574; PMCID: PMC5349390. https://pubmed.ncbi.nlm.nih.gov/27821574/
- Köhli PC, Hambrecht J, Zhu J, Chiapparelli E, Schönnagel L, Guven AE, Duculan R, Otto E, Kienzle A, Evangelisti G, Shue J, Tsuchiya K, Burkhard MD, Mancuso CA, Sama AA, Girardi FP, Cammisa FP, Hughes AP. Undetected low bone mineral density in patients undergoing lumbar fusion surgery-prevalence and risk factors. N Am Spine Soc J. 2025 Jan 31;21:100591. doi: 10.1016/j.xnsj.2025.100591. PMID: 40041543; PMCID: PMC11876750. https://pubmed.ncbi.nlm.nih.gov/40041543/
- Lane JM, Serota AC, Raphael B. Osteoporosis: differences and similarities in male and female patients. Orthop Clin North Am. 2006 Oct;37(4):601-9. doi: 10.1016/j.ocl.2006.09.002. PMID: 17141018. https://pubmed.ncbi.nlm.nih.gov/17141018/
- Lane JM, Russell L, Khan SN. Osteoporosis. Clin Orthop Relat Res. 2000 Mar;(372):139-50. doi: 10.1097/00003086-200003000-00016. PMID: 10738423. https://pubmed.ncbi.nlm.nih.gov/10738423/
- Lewiecki EM, Bilezikian JP, Clark A, Collins MT, Kado DM, Lane JM, Langdahl B, McClung MR, Snyder PJ, Stein EM. Proceedings of the 2024 Santa Fe Bone Symposium: Update on the Management of Osteoporosis and Rare Bone Diseases. J Clin Densitom. 2025 Jan-Mar;28(1):101559. doi: 10.1016/j.jocd.2024.101559. Epub 2024 Dec 28. PMID: 39826229. https://pubmed.ncbi.nlm.nih.gov/39826229/
- Russell LA. Management of difficult osteoporosis. Best Pract Res Clin Rheumatol. 2018;32(6):835-847. doi:10.1016/j.berh.2019.04.002. https://pubmed.ncbi.nlm.nih.gov/31427058/