Can Knock Knees Be Corrected in Adults?

Knock knee is an improper alignment of the knee joint. In adults, it can lead to knee pain and premature degeneration of the knee joint.
What are knock knees?
Knock knee is a condition in which the knees bend inward toward one another. In significant cases, the knees touch or "knock" against one another, even when a person is standing with their ankles apart.
What causes knock knees?
There are many causes for genu valgum (knock knees). Most cases are congenital, where people are born with the deformity, and it becomes more noticeable with time. An injury to the growth plate in childhood can also lead to knock knees. Knock knees can be surgically corrected. The surgical technique used may vary depending on age.

What impact do knock knees have on the knees, hips and ankles?
Knock knees can cause the kneecaps to be off-center, which increases pressure and pain in the front of the knee. Knock knee alignment places high stresses on the outside (lateral side) of the knee, causing additional knee pain. These stresses often lead to knee arthritis. Abnormal hip rotation is often associated with knock knees and can cause hip pain. This needs to be recognized and addressed with any corrective surgery for the knock knees. The ankles may struggle to keep the foot flat on the ground. The ankle and foot will need to compensate to make up for misalignment at the knee, often leading to ankle pain.
I have knock knees as well as hip and back pain. Is there any correlation?
Knock knees can be associated with hip and back pain, and correction of the deformity will often alleviate this pain. If a patient is overweight and has knock knees, then losing weight will help the hip and back pain. Knock knees can create leg length differences. A leg length discrepancy will also frequently lead to hip and back pain. Having the leg lengths equalized will help treat the pain. The treatment approach can be tailored to address the leg lengths.
I have knock knees and kneecap instability. Is that a thing?
Yes, knock knees is often associated with patellar maltracking or instability. Symptoms can vary from kneecap pain to a dislocating knee cap. This is known as complex patellofemoral instability. The only way to fix the patellar alignment and knee pain is to correct both the direction of pull of the patellar tendons and fix the knock knee.
Can knock knees get worse over time?
The deformity can get worse over time. In children the deformity can progress with growth. If arthritis is present, the deformity can progress as the joint wears out further. In adults the medial ligaments of the knee can stretch and cause greater deformity. Fixing the problem early will avoid progression of this condition.
Are there any nonsurgical treatments for knock knees?
The best nonsurgical treatments for patients with knock knees are aimed at reducing other risks of arthritis development in the knee. This includes maintaining a normal body weight, keeping fit while avoiding high impact activities (running, soccer, singles, tennis, basketball, etc.) and, if arthritis is already present, wearing an unloader knee brace. These treatments will not change the knock knee deformity but they will help in slowing the progression of degeneration.
Surgery may be recommended if your condition is causing you physical and/or emotional health problems, or putting you at risk for early onset osteoarthritis or other complications. Talk with a physician about the best treatment for you.
What are the surgical treatments for knock knees?
There are two main surgeries to treat knock knees: A distal femoral osteotomy (DFO), or a DFO combined with a high tibial osteotomy (an osteotomy of the proximal tibia).
Distal femoral osteotomy, or DFO, surgery involves creating a cut in the femur just above the knee to reshape the bone and realign the entire limb. This bony surgery is stabilized with a strong plate and screws placed deep to the skin and muscle. Patients are admitted into the hospital for about two nights after the surgery. Rehabilitation begins right away with partial weight bearing and range of motion exercises and continues for several weeks.
When the magnitude of the knock knee deformity is large (above 12 degrees), the patient usually requires osteotomy of both the femur and the tibia. The distal femoral osteotomy is the same as described above. The high tibial osteotomy will correct the portion of the valgus that originates in the lower leg. Sometimes this osteotomy is fixed with a plate and screws similar to the DFO. Other times the tibia osteotomy is fixed with an intramedullary nail. The decision is made based on careful preoperative planning and analysis of the shape of the bones.
As with the DFO, patients undergoing femur and tibia surgery are admitted into the hospital for about two nights after the surgery. Rehabilitation begins right away with partial weight bearing and range of motion exercises and continues for several weeks. The recovery time does not change with this combined surgery.
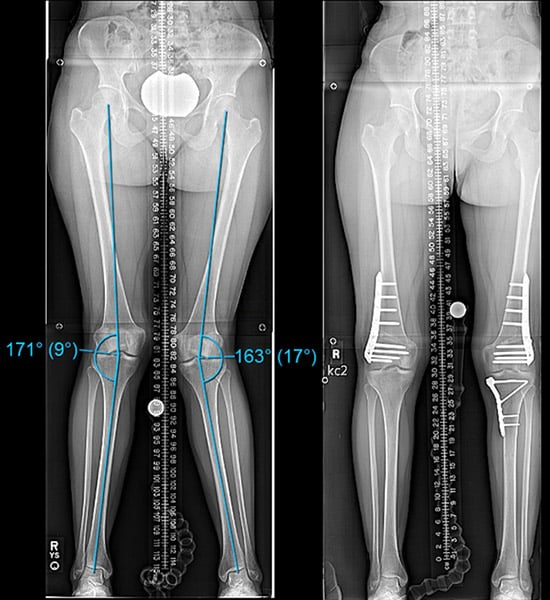
Front-to-back X-rays of a patient with a 9-degree valgus angulation in the right leg (shown left in image) and a 17-degree angulation in the left leg. The right side was able to be corrected with a DFO, but the left side required combined DFO and high tibial osteotomy using plates.
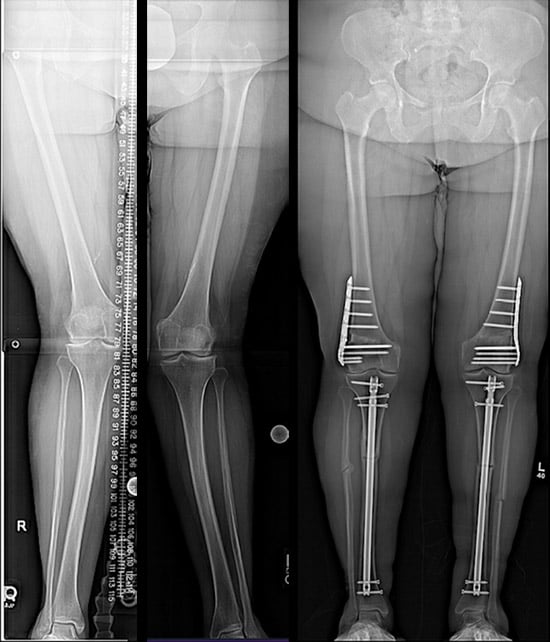
In the patient shown in these X-rays, the middle of each tibia bone had a swerve or bow that was best corrected with an intramedullary nail. The femurs were treated with the DFO using plates.
Is knock knee surgery possible for someone in their late twenties?
There is no fixed age limit for corrective surgery for knock knees. The surgical technique used may vary depending on age. Children can take advantage of their remaining growth to guide the bones straighter with minor surgery. Adults can benefit from osteotomy surgery on the knee to obtain a correction. Patients over sixty years of age may receive a different type of osteotomy than younger patients to ensure timely healing. Older patients with arthritis will often receive a knee replacement to treat both problems. It is important to consult with a physician to determine the best course of treatment.
