Medial Patellofemoral Ligament (MPFL) Reconstruction

What is the medial patellofemoral ligament (MPFL)?
The medial patellofemoral ligament (MPFL) is a part of the complex network of soft tissues that stabilize the knee. The MPFL attaches the inside part of the patella (kneecap) to the long bone of the thigh, also called the femur.
Together, the patella and femur compose the patellofemoral joint.
Injury to the MPFL can occur when the patella dislocates or becomes subluxated (partially dislocated) often due to a sports injury or in some cases due to a twisting or pivoting event. These incidents are more common in patients with anatomic predispositions such as patella alta (a high kneecap), loose joints (ligamentous laxity) and a less constrained or flatter patellofemoral joint. People with these injuries are described as having patellofemoral instability. Patellar instability is seen more often in females than males.
What is MPFL reconstruction?
MPFL reconstruction is a surgery in which a new medial patellofemoral ligament is created to stabilize the knee and help protect the joint from additional damage. It offers an excellent treatment option for people who have experienced one or more dislocation.
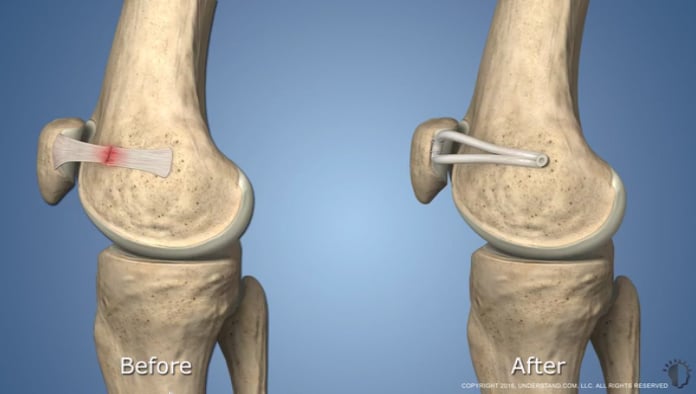
Injury to the MPFL
In the healthy knee, the patella glides smoothly within its groove (the trochlea) on the femur as the joint is flexed or extended. The MPFL plays a particularly important role in keeping the patella in the groove by acting like a leash that restrains the patella's movement.
When a patellar dislocation occurs, soft tissues are damaged as the patella “jumps” the track and then comes forcibly back into place. Because the kneecap dislocates toward the outside of the leg, the ligament on the inside of the knee (the MPFL) is stretched or torn.
Left untreated, an injured MPFL can sometimes heal on its own. However, the ligament may not heal, or it may heal in a loosened or lengthened position. This can predispose the patella to dislocate again in the future. Repeat dislocations subsequently increase the risk of damage to the cartilage of the knee. While the pain and swelling associated with a dislocated kneecap are a disability, the greater concern is subsequent injury to the cartilage. Cartilage covers the ends of the bones where they meet in the knee joint, and once damaged, there is a risk of developing patellofemoral arthritis, a significantly more difficult condition to treat. For this reason, it is always advisable to get treatment that will help prevent further dislocations of the kneecap.
Video: MPFL reconstruction animation
Watch this animation to understand how MPFL reconstruction surgery works.
What is the reconstruction protocol for MPFL?
At the Patellofemoral Center at HSS, patients with patellar instability undergo a thorough assessment that includes a physical examination and review of the patient's medical history. A magnetic resonance imaging (MRI) is also performed to help the doctor understand the condition of the cartilage in the patellofemoral joint and helps determine whether the patient is a candidate for MPFL or a bony procedure, such as tibial tubercle transfer.
Although non-operative treatment does not have a significant role in the treatment of recurrent patellar instability, in cases where the patient has experienced a single dislocation without any cartilage injury revealed on an MRI, he or she may be treated with bracing and physical therapy. Patients undergoing MPFL reconstruction receive regional anesthesia – a spinal nerve block that numbs the lower half of the body – and sedation through an IV. The orthopedic surgeon then replaces the injured ligament with a portion of a tendon taken either from the patient’s own hamstring or from donor tissue.
An arthroscope is used to view the inside of the knee, and the ligament reconstruction is conducted using two small incisions. The entire surgery takes about an hour, and patients return home the same day, with their knee stabilized in a brace.
MPFL reconstruction produces excellent results and has a very low rate of complication. Rare complications, however, can occur including fractures, infections or blood clots. The procedure can be performed safely in children with open growth plates (the area where bone grows), as opposed to surgical approaches that change bone alignment and which are not appropriate in young patients. With no alternative available, in the past, children were sometimes placed in a brace, but remained at risk for additional dislocations until they reached skeletal maturity, at which time a surgical reshaping of the bone (osteotomy) would become an option. Today, MPFL reconstruction is a safe option for children and teenagers.
MPFL reconstruction as a revision to prior, unsuccessful surgeries
Orthopedic surgeons at the Patellofemoral Center also perform MPFL reconstruction on patients who have had other, less successful surgeries to address the condition. Such prior surgeries may include:
- Arthroscopic, minimally invasive surgery in which torn tissue in the patellofemoral joint is “cleaned up.”
- Medial imbrication, a procedure in which the surgeon tightens the MPFL by taking a “tuck” in it, similar to tightening a garment.
- Lateral release, in which the ligament on the outside part of the patellofemoral joint is loosened.
Although a lateral release alone is not an effective surgical option for patellar instability, this procedure may be done in conjunction with an MPFL reconstruction to address other problems in the joint and to restore balance in the knee.
Tibial tubercle transfer or osteotomy may also be done in conjunction with an MPFL in patients who have significant malalignment of the patellofemoral joint. This procedure is recommended for patients who have an anatomical abnormality in which the patella tendon attaches to the tibia in such a way that there is a significant lateral (outward) pull on the patella.
What to expect after MPFL reconstruction
Immediately following MPFL reconstruction, patients can bear weight on the affected leg, which is placed in a brace that is worn for 4 to 6 weeks. The brace keeps the leg straight during walking until there is good control of the quadriceps. Physical therapy begins within the first two weeks of surgery and is extremely important throughout the entire recovery. Other measures that may be recommended include devices that provide electric stimulation to the muscles around the knee and an ice machine that compresses and cools the leg, thereby reducing swelling and pain. (Insurance may not cover the cost of these devices.)
Most people can generally return to sport or play sometime between 4 to 7 months after MPFL reconstruction. If you are considering the surgery, be aware that recovery times may vary and can be dependent on your individual anatomy, capacity to heal and general health prior to surgery.
Authors


References
- Liu JN, Brady JM, Kalbian IL, Strickland SM, Ryan CB, Nguyen JT, Shubin Stein BE. Clinical Outcomes After Isolated Medial Patellofemoral Ligament Reconstruction for Patellar Instability Among Patients With Trochlear Dysplasia. Am J Sports Med. 2018 Mar;46(4):883-889. doi: 10.1177/0363546517745625. Epub 2018 Jan 3. PMID: 29298083.
- Liu JN, Steinhaus ME, Kalbian IL, Post WR, Green DW, Strickland SM, Shubin Stein BE. Patellar Instability Management: A Survey of the International Patellofemoral Study Group. Am J Sports Med. 2018 Nov;46(13):3299-3306. doi: 10.1177/0363546517732045. Epub 2017 Oct 6. PMID: 28985094.