Primary Transtibial Amputation with Simultaneous Osseointegration for Congenital Ankle Deformity
From Grand Rounds from HSS: Management of Complex Cases | Volume 15, Issue 1
Case Report
A 43-year-old man, working as a garden supply laborer, presented with a year of persistent left ankle pain after open reduction and internal fixation for a motorcycle injury. (The patient gave his permission to share identifying details of his story.) He had been told as a child he had an atypical ankle, for which he had external fixator lengthening. His ankle was constantly painful prior to the motorcycle injury and worse since. He also had lateral knee pain. He was aware of osseointegration and asked if he was eligible for this rehabilitation option.
Examination (Figure 1) was notable for a valgus left foot and ankle, with reduced muscle bulk versus the right. His gait was antalgic on the left with minimal knee flexion throughout and no ankle push off (Video 1). Radiographs showed the left leg to be 4 cm shorter than right, with genu valgum, malunion of the lengthened tibia, the recently placed distal tibia fixation, and a ball and socket ankle with short fibula featuring nonunion and malunion at different locations, characteristic of fibular deficiency. He was counseled that a pain-free limb could be provided via reconstructions including hardware removal, distal tibia osteotomy, hindfoot fusion, distal femur osteotomy, and lengthening. He wanted a faster option for painless, high-demand function and asked if he could have tibial osseointegration instead. This was indeed a reasonable option for him. He elected to defer distal femur osteotomy unless the knee remained symptomatic.


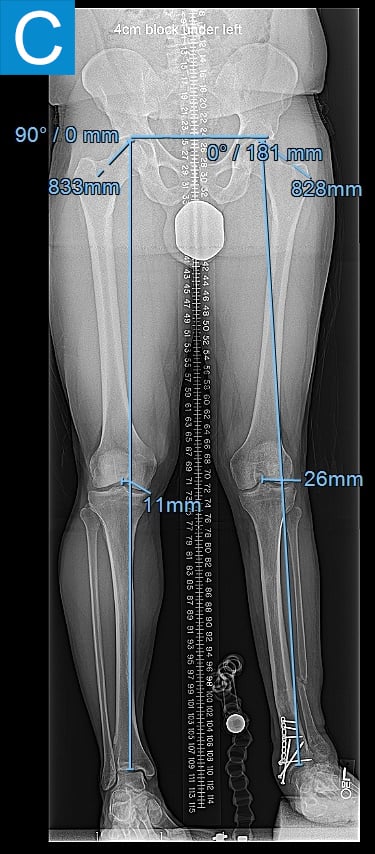

Figure 1. Preoperative clinical photos and radiographs. (A) Front and (B) rear views of the patient show a short left leg with foot and ankle valgus and genu valgum and a left calf with reduced musculature. (C) Standing coronal and (D) lateral tibia radiographs depict the prior distal tibia lengthening with fibula nonunion, ankle fracture with fixation, ball and socket ankle, and short fibula. Also note the genu valgum.
Video 1. Preoperative gait demonstration.
His first surgery was the transtibial amputation with simultaneous osseointegration. This entailed performing amputation of the tibia and fibula at the planned level, reaming and broaching the tibial canal to achieve a uniform canal for the diameter and length of the implant and inserting the osseointegration implant. This feels similar to how a cementless total hip femur implant mixed with an intramedullary nail might feel. Phantom nerve pain was prevented via regenerative peripheral nerve interface technique. Then the skin around the implant that passed through the skin portal was closed. His recovery followed the standard protocol of 4 weeks non-weightbearing followed by 4 weeks of progressive loading, with the prosthesis attached at 2 months (Figure 2). He quickly achieved a better gait than he had prior to amputation (Video 2) with essentially equal swing and stance per leg, but lateral knee pain persisted. Four months after osseointegration, a distal femur osteotomy was performed to neutralize his alignment.



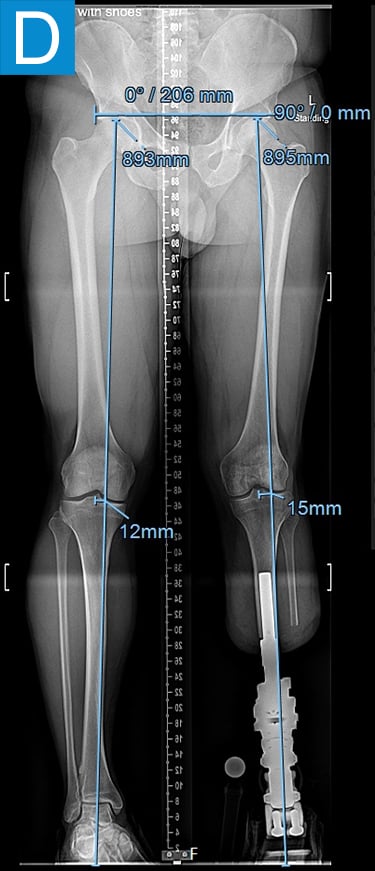
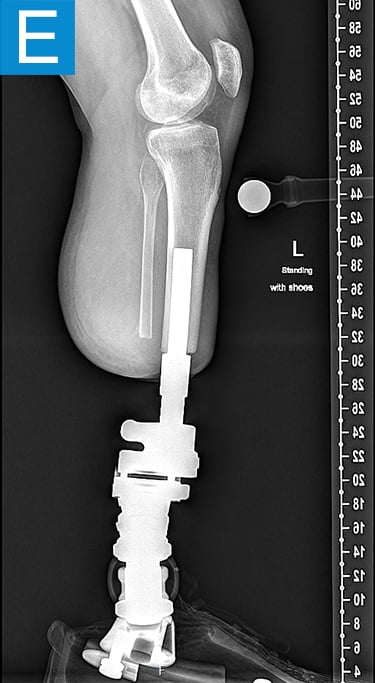

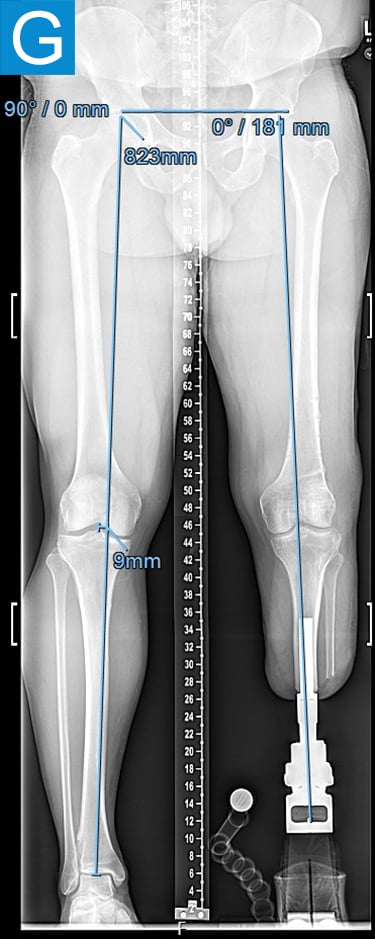
Figure 2. Postoperative clinical photos and radiographs. (A) Front and (B) rear views show the patient standing with the osseointegrated tibia prosthesis. (C) Photo shows stable and healthy skin at portal site to be, although slightly dry due to the winter weather. The gold-colored metal is part of the permanent transcutaneous implant; the shiny silver-colored metal beneath the gold is part of the clinician-removable prosthesis connector, and the matte silver metal beneath features a screw at the front, by which the patient secures the prosthesis. (D) Standing coronal radiograph depicts residual genu valgum in the osseointegrated leg. (E) Lateral radiograph of the osseointegrated tibia. (F) Coronal radiograph of the left knee shows the distal femur osteotomy. (G) Final coronal radiograph after distal femur plate and screw removal shows well-aligned left leg with osseointegrated prosthesis.
Video 2. Postoperative gait demonstration after osseointegration, before distal femur osteotomy.
The patient was able to resume heavy labor (Video 3) 7 months after the amputation and osseointegration and 4 months after the distal femur osteotomy. Now, 2.5 years after the osseointegration, he has maintained a demanding work schedule, 6 to 7 days per week for 8 to 9 months per year. He averages over 20,000 daily steps, has no pain, and has missed no workdays.
Video 3. Patient demonstrating pulling heavy racks of landscaping supplies.
Bonus Video 4.
Discussion
Awareness has increased, particularly in the last decade, of titanium transcutaneous osseointegration nail (TiTON) surgery as a rehabilitative option since its first clinically successful use in 1990 [1,2]. Our practice has performed over 125 tibia osseointegration procedures since introducing the technique to HSS in 2017. Outcomes have been nothing short of remarkable, with patients showing consistent improvements in mobility, as measured by prosthesis use, timed walking distance, and surveyed quality of life [3,4]. Patients often report they wear the prosthesis from waking to sleeping, with some transtibial osseointegration patients even wear it to sleep. Patients rarely report removing the leg during the day, which enables improved mobility without the extended routine familiar to patients with a socket prosthesis [5].
Our group has refined surgical techniques [6] for osseointegration performed at the time of primary amputation in patients with full limbs like this patient; for existing amputees who are dissatisfied with their socket rehabilitation, revision amputation and osseointegration are an option. We have also solidified a rehabilitation routine[7,8] that allows patients to walk at around 2 to 3 months after surgery, as soon as the prosthesis is attached [9]. Any prosthesis can be attached to the standardized connector, and routine hygiene involves a regular daily shower with gentle wiping of the skin-implant portal. We recommend a couple of visits to the prosthetist annually for routine maintenance. Patients achieve a surprisingly near-native activity level, with many enjoying golfing, ballroom dancing, cycling, rock wall climbing, swimming, and even completing marathons.
While a series of procedures could have retained this patient’s leg, he was frustrated by its poor lifelong function and reports both excellent mobility and improved quality of life with osseointegration. This case of primary amputation of a patient with a chronically painful foot and ankle deformity, including deformity at other locations, illustrates a potential option for other patients with challenging or unsalvageable foot and ankle conditions, such as severe Charcot arthropathy, infected total ankle arthroplasty, complex regional pain syndrome, or diabetic and vascular disease.
Authors

References
- Hoellwarth JS, Tetsworth K, Rozbruch SR, Handal MB, Coughlan A, Al Muderis M. Osseointegration for amputees: current implants, techniques, and future directions. JBJS Rev. 2020;8(3):e0043. doi:10.2106/JBJS.RVW.19.00043
- Hoellwarth JS, Tetsworth K, Akhtar MA, Al Muderis M. The clinical history and basic science origins of transcutaneous osseointegration for amputees. Adv Orthop. 2022;2022:7960559. doi:10.1155/2022/7960559
- Reif TJ, Khabyeh-Hasbani N, Jaime KM, Sheridan GA, Otterburn DM, Rozbruch SR. Early experience with femoral and tibial bone-anchored osseointegration prostheses. JB JS Open Access. 2021;6(3):e21.00072. doi:10.2106/JBJS.OA.21.00072
- Muderis MA, Tan YC, Lu W, et al. Transtibial osseointegration following unilateral traumatic amputation: An observational study of patients with at least two years follow-up. Injury. 2024;55(6):111568. doi:10.1016/j.injury.2024.111568
- Page BJ, Sheridan GA, Greenstein MD, Hoellwarth JS, Reif TJ, Rozbruch SR. PLUS-M mobility values of osseointegration patients: How do osseointegration limb replacement prosthesis users compare to traditional socket amputee prosthesis users? Ho Am J Phys Med Rehabil. 2025;104(8):687-692. doi:10.1097/PHM.0000000000002685
- Geiger EJ, Hoellwarth JS, Reif TJ, Rozbruch SR. Osseointegration of the tibia after a primary amputation. JBJS Essent Surg Tech. 2022;12(4):e22.00005. doi:10.2106/jbjs.st.22.00005
- Grunfeld M, Reif TJ, Rozbruch SR, Hoellwarth JS. Lower extremity osseointegration postoperative rehabilitation protocols: A scoping review. Phys Ther. 2025;105(1):zae139. doi:10.1093/ptj/pzae139
- Melton D, Prasso L, Abernethy A, Hoellwarth JS, Strickland T. Consensus statement on prehabilitation and rehabilitation of osseointegration patients. OTA Int. 2025;8(1 Suppl):e371. doi:10.1097/OI9.0000000000000371
- Kafedzic H, Rozbruch SR, Reif TJ, Hoellwarth JS. Constructing an osseointegrated prosthetic leg. JBJS Essent Surg Tech. 2024;14(1):e22.00064. doi: 10.2106/JBJS.ST.22.00064.