Bilateral Transtibial Osseointegration Limb Replacement in a 36-Year-Old Quadrilateral Amputee after Sepsis
From Grand Rounds from HSS: Management of Complex Cases | Volume 15, Issue 1
Case Report
A 36-year-old woman, a quadrilateral amputee who used bilateral upper- and lower-extremity socket prostheses, presented for consideration of bilateral lower-extremity osseointegration (Figure 1). (The patient gave her permission to share identifying details of her story.) Following postpartum endometritis in 2016, she had undergone bilateral transtibial and transradial amputation secondary to sepsis and disseminated intravascular coagulation (DIC). These procedures required extensive bilateral lower-extremity skin grafting.

Figure 1. A: Clinical image of patient showing bilateral upper and lower limb socket prostheses. B: Clinical image from front of bilateral tibia showing scarring. C: Clinical image from side showing bilateral tibia.
She reported constant aching and dull pain rated at 5/10, worsened by standing, walking, stair climbing, and performing daily activities, that improved with rest and activity modification. She had struggled with sockets and reported no phantom limb pain. Clinical examination found extensive scarring and skin grafts over bilateral tibias and femurs, with fissuring and tight, shiny skin. Small pressure wounds were noted on the left stump and on the medial aspect of the right stump. She had full extension of both knees with flexion to 100° on the right and 110° on the left. She had full power, no instability, and no neurological deficits. X-rays showed approximately 12 cm residual tibia bilaterally, with no deformity in the tibia, knee joint, or femur (Figure 2).
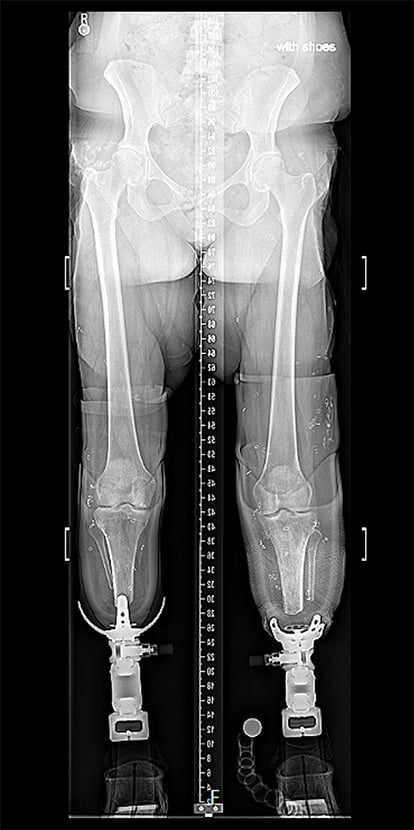
Figure 2. X-ray of patient’s bilateral lower limbs with patient standing in socket prostheses.
The patient was considered an excellent candidate for bilateral tibial osseointegration using a percutaneous technique. Her challenges included compromised skin quality due to previous skin grafting and difficulty doffing and donning the limb prosthesis given her bilateral upper limb prostheses. We worked with a prosthetist to make adapters for the osseointegration prosthetic limbs to be compatible with her socket upper limbs. CT scans were ordered, and custom prostheses were made.
The custom-made tibial prostheses were designed to be inserted by impaction after reaming up to the appropriate diameter (Figure 3). This was a bilateral surgery with the right side and left side in succession. Considerable care was taken when handling her soft tissues due to poor skin quality. A percutaneous technique was used [1]. First, a 2.4-mm Steinmann pin was placed under fluoroscopy; next, a small 18-mm stoma was created. The tibial canal was sequentially reamed up to 19 mm in the distal 2 cm of her tibia. Then it was serially rasped and broached, increasing by 1 mm at a time, until 19 mm was achieved proximally at 100 mm, which was the planned length of the implant. The patient did not require peripheral nerve surgery such as target muscle reinnervation or regenerative peripheral nerve interface surgery.
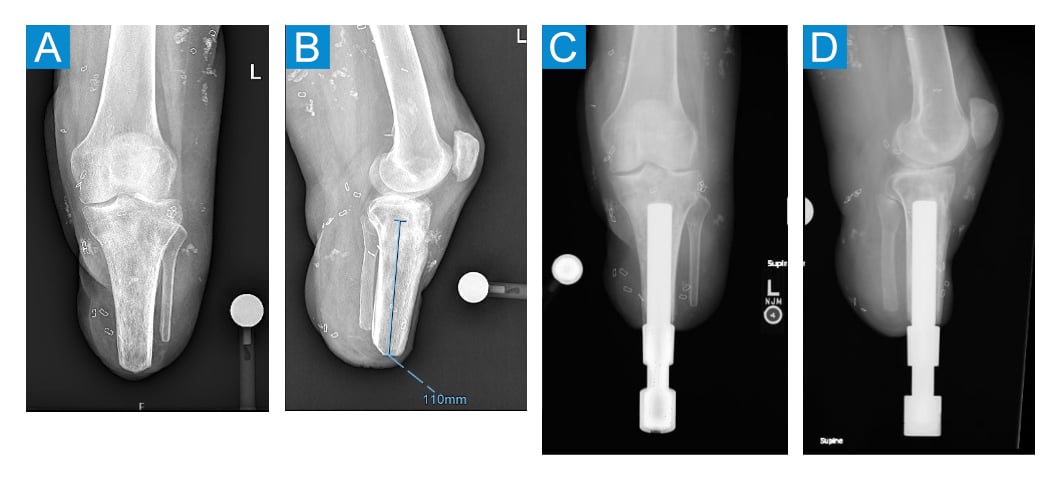
Figure 3. A: Preoperative anteroposterior (AP) X-ray of left leg. B: Preoperative lateral X-ray of left leg. C: Postoperative AP X-ray of left leg. D: Postoperative lateral X-ray of left leg.
Routinely, patients remain hospitalized for 1 or 2 days for analgesia and to learn the stoma care techniques. The initial postoperative protocol is a non-weightbearing period of 5 to 6 weeks, after which time the patient begins the loading process using a rubber footie attached to the prosthesis. Standing on an analogue weighing scale, the patient’s initial goal is to achieve a weight of 20 or 30 lbs (titrated to their own starting body weight) and add on 5 lbs every day until 100% or more of their body weight is reached over 5 to 6 weeks. This is done for 10-to-15-minute intervals 4 to 6 times a day. Usually, the rubber footie and eventually the prosthetic limb are attached to the dual cone with the aid of a torx wrench, although for our patient we had to take into consideration her upper limb sockets. Patients will use a torx wrench to doff and don the footie as a precursor to doffing and donning the prosthesis. This would not be possible for our patient, so a lever was added to her prosthesis to facilitate her needs. It was vital to have a prosthetist work with the patient [2].
She attended rehabilitation and completed the loading phase with the assistance of an adapted upper limb walker. Her prosthetist adapted her dual cone prosthetic so that she could doff and don it without using a torx wrench, which would be standard. Instead, she used a clip lever, similar to a bicycle seat attachment. She is now 15 months post-surgery and has achieved a high level of independent ambulation (Figure 4, Video 1). She no longer suffers from socket pain, and she is more independent in her activities of daily living, including caring for her young family (Video 2).

Figure 4. Clinical image showing patient standing with her new osseointegration and prosthesis.
Video 1: Clinical video of patient using her upper limb sockets to doff and don her prosthetic limb.
Video 2: Clinical video of patient using both prosthetics to walk and use an agility ladder. This highlights the functional gains patients can make in terms of agility with appropriate rehabilitation.
Discussion
Patients who have osseointegration limb replacements generally have higher patient reported outcome measures on specific scores compared to socket users [3]. The current indications for osseointegration include patients who have difficulty wearing sockets, pain, very short residual segments, and struggles with the skin around the sockets [4]. The challenges for patients undergoing osseointegration include managing nerve-related and soft-tissue pain. There are well described techniques in reducing nerve-related pain in the setting of amputation [5]. Osseointegration is an evolving field in which customization is possible, and it is important to consider patient indications and needs before offering this surgery.
Authors

References
- Hoellwarth JS, LoPolito AG, Greenstein MD, Reif TJ, Rozbruch SR. Percutaneous exposure for tibia osseointegration: reduced antibiotics, improved perioperative metrics, and greater pain reduction versus open exposure. OTA Int. 2025;8(4):e428. doi: 10.1097/OI9.0000000000000428.
- Kafedzic H, Rozbruch SR, Reif TJ, Hoellwarth JS. Constructing an osseointegrated prosthetic leg. JBJS Essent Surg Tech. 2024;14(1):e22.00064. doi: 10.2106/JBJS.ST.22.00064.
- Page BJ, Sheridan GA, Greenstein MD, Hoellwarth JS, Reif TJ, Rozbruch SR. PLUS-M mobility values of osseointegration patients: how do osseointegration limb replacement prosthesis users compare to traditional socket amputee prosthesis users? Am J Phys Med Rehabil. 2025;104(8):687-692. doi: 10.1097/PHM.0000000000002685.
- Hoellwarth JS, Tetsworth K, Rozbruch SR, Handal MB, Coughlan A, Al Muderis M. Osseointegration for amputees: current implants, techniques, and future directions. JBJS Rev. 2020;8(3):e0043. doi: 10.2106/JBJS.RVW.19.00043.
- Vaeth AM, Black GG, Vernice NA, et al. Soft-tissue contouring and nerve management during lower-limb osseointegration surgery. JBJS Essent Surg Tech. 2025;15(2):e22.00074. doi: 10.2106/JBJS.ST.22.00074.