Lumbar Fusion

When lower back pain and/or related leg pain are not relieved by conservative treatments such as activity modification, medications, physical therapy, epidural steroid injections, nerve ablation procedures, or other conservative therapies, some surgical options are available.
Depending on the cause of your pain, the appropriate surgical treatment will take the form of spinal decompression, lumbar fusion, or a combination of the two.
There are a wide variety of approaches to lumbar fusion surgery. Which option is best for each you can be determined by consulting with a spine surgeon.
- What is a lumbar fusion?
- What are the different types of lumbar fusion?
- What is the recovery time after lumbar fusion surgery?
What is a lumbar fusion?
Lumbar fusion broadly refers to various spinal surgery techniques that connect two or more vertebrae in the lumbar spine (lower back). In general, fusion surgery (also known as arthrodesis) is designed to cause two or more bones to grow together into one, single bone. Lumbar fusions reduce the motion between two or more vertebrae to alleviate pain caused by various conditions, such as degenerative disc disease or spondylolisthesis.
Fusion procedures may also be performed at the same time as some spinal decompression procedures to provide stability. For example, when a large portion bone material must be removed to decompress the affected area, the spine could later become unstable unless a fusion is also performed. (Find a surgeon at HSS who performs lumbar spinal fusion.)
Spine anatomy
The spinal cord extends from the base of the brain and enters the spinal canal, a protective space within our bony spine, to carry signals to and from the brain throughout the body. The spine is divided into three sections, named for their location and function:
- The cervical spine composes the body’s neck and allows body to turn the head in many directions.
- The thoracic spine supports the rib cage, protecting the heart, lungs, and large vessels.
- The lumbar spine connects the torso to the pelvis and allows the body to bend, flex, and twist around the torso.
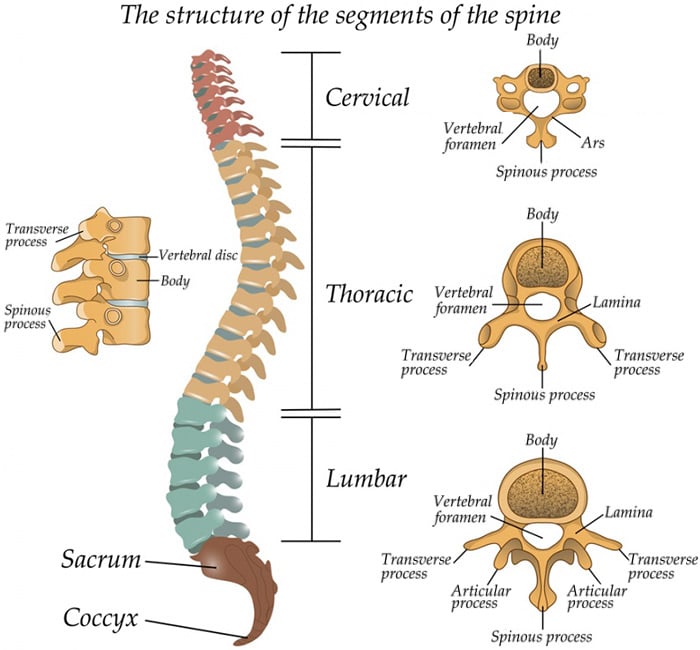
Lateral (side) view of the spine in a person facing left.
What are the different types of lumbar fusion?
There are numerous techniques to achieve fusion in the lumbar spine, and they break down into three basic categories:
- posterior and posterolateral fusion (PLF) procedures
- lumbar interbody fusion (LIF) procedures
- lumbar corpectomy and vertebral body replacement
Posterior spinal fusion and posterolateral fusion (PLF)
Both of these types of procedures have been utilized in spine surgery since it was first developed. The techniques use bone grafting placed along the posterior (back) or posterolateral (back and sides) of the spine to produce a fusion. In modern surgery, the grafts are supplemented with screws or other hardware to connect the vertebrae while the bones heal.
A posterior fusion or PLF surgery is commonly performed in conjunction with a spinal decompression surgery such as a lumbar laminectomy and/or discectomy to reduce pressure on the spinal nerve.
Lumbar interbody fusion (LIF) surgeries
LIF procedures involve placing an implant, commonly referred to as a “cage,” in the disc space between two vertebra. The cages come in a wide variety of shapes, sizes, and materials, depending on the method of insertion and goals of the surgery. These cages stabilize the spine until the bone grows together to achieve fusion of the vertebrae. In many cases the interbody fusion is supplemented with a conventional posterolateral fusion.
Lumbar interbody fusions have numerous subtypes, chiefly named for the direction or point on the body from which the spine will be accessed during surgery. For example, in an anterior lumbar interbody fusion (ALIF), the spine is accessed through the "anterior" (front or abdomen region) of the body. LIF surgeries include:
- anterior lumbar interbody fusion (ALIF)
- posterior interbody fusion
- posterior lumbar interbody fusion (PLIF)
- transforaminal lumbar interbody fusion (TLIF)
- minimally invasive PLIF or TLIF surgeries (MIS-PLIF or MIS-TLIF)
- lateral lumbar interbody fusion (LLIF)
- oblique lumbar interbody fusion (OLIF)
Anterior lumbar interbody fusion (ALIF)
This surgery is performed to remove the degenerated disc that may be part of the source of back or leg pain. This procedure restores the space between the vertebral bodies, relieving pressure and creating more room for spinal nerves to exit. It is called an anterior procedure because the spine is approached from the front. Unlike posterior approaches (from the back), the anterior approach avoids damage to the low back muscles and direct contact with nervous structures. The removed disc is replaced with an implant and bone grafting materials. The adjacent vertebral bodies then fuse together over time.

Learn more by visiting the page, ALIF Surgery: Anterior Lumbar Interbody Fusion.
Posterior lumbar interbody fusion (PLIF)
A posterior lumbar interbody fusion (PLIF) is performed to remove a disc that is the source of back or leg pain (as in the case of sciatica) and fuse spinal vertebrae with bone graft. It is called a posterior procedure because the spine is approached through an incision on the back. Instrumentation in the form of screws and rods is used to help stabilize the spine.
Learn more by visiting the page, PLIF Surgery: Posterior Lumbar Interbody Fusion.

Minimally invasive PLIF
In some patients who require PLIF surgery, there may be an opportunity to use minimally invasive PLIF techniques (MIS-PLIF). MIS-PLIF uses smaller incisions and less tissue dissection to achieve similar results of traditional, open surgery.
Learn more by visiting the page, PLIF Surgery: Posterior Lumbar Interbody Fusion.
Transforaminal lumbar interbody fusion (TLIF)
As in the posterior lumbar interbody fusion (PLIF) procedure, an implant and bone graft are used to fuse the spinal vertebrae after the disc is removed. A TLIF procedure involves removing some or all of the bony facet joint in addition to the intervertebral disc. Inserting the graft from the side where the facet joint has been removed is done to avoid moving or damaging nerve roots during the procedure. Learn more by visiting the page, TLIF Surgery: Transforaminal Lumbar Interbody Fusion.
Minimally invasive TLIF
Using minimally invasive surgery (MIS), transforaminal lumbar interbody fusion (MIS-TLIF) can be done in certain patients with smaller incision than traditional open spinal surgeries, decreasing damage to the low back muscles. Learn more by visiting the page, TLIF Surgery: Transforaminal Lumbar Interbody Fusion.

Lateral lumbar interbody fusion (LLIF)
This procedure, also known as lateral access spine surgery, is a minimally invasive surgery that accesses the spine from incisions on the side of the body. This procedure avoids separating the low back muscles, cutting bone, or moving aside blood vessels as required for other minimally invasive spine fusion procedures (PLIF, TLIF, ALIF). Lateral access spine surgery can treat a variety of conditions including herniations, asymmetric disc degeneration (degenerative scoliosis), nerve impingement, certain tumors, as well as instability and pain resulting from disc degeneration.

Learn more by visiting the page, LLIF/XLIF Surgery: Lateral Lumbar Interbody Fusion.
Oblique lumbar interbody fusion (OLIF)
Oblique lumbar interbody fusion (OLIF) is a variation of lateral access surgery. Where the LLIF surgery involves dividing the psoas muscle, which lies along the sides of the lumbar spine, the OLIF spares this muscle. OLIF is also referred to as “anterior to the psoas" surgery because the spine is accessed in front of the psoas muscle, which runs from the lower spine across the pelvis. This procedure can be used to achieve similar results to LLIF in some patients.
Learn more by visiting the page, Minimally Invasive Lower Back Surgery for Disc Degeneration: The Anterolateral (Side) Approach.
Lumbar corpectomy and vertebral body replacement
Vertebral body replacement (VBR) is a rarely used spinal fusion procedure that involves removing an entire vertebra from the spine (corpectomy) and replacing it with an implant or bone graft.
What is the recovery time after lumbar fusion surgery?
Because there is a wide variety of surgical techniques for achieving vertebral fusion in the lumbar spine, so, too, is there some variety in recovery times. For example, a minimally invasive LLIF recovery can be much shorter than a PLIF. Recovery times will differ both by procedure and by individual patient. Recovery expectations should be discussed with your surgeon. (Find a surgeon at HSS who performs lumbar spinal fusion.)
Why choose HSS for lumbar decompression and fusion surgery?
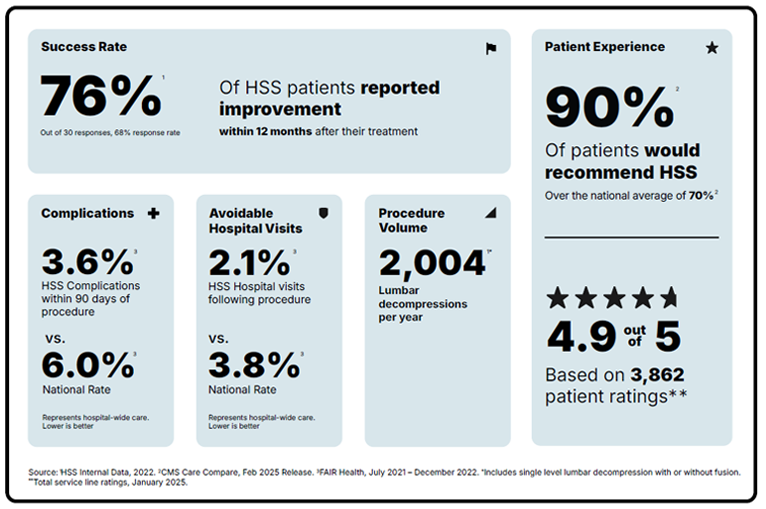
Lumbar spinal decompression with fusion is a surgery focused on reducing pain and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding these data points will help you make the best decision for your care: See hospital reliability data
Authors

Explore Related Patient Stories
View All Patient Stories
Janet Schiel-Jackson
Carmel, NY
Lumbar Fusion

Micky Padway
New York, NY
Lumbar Fusion
Katherine Toland
Princeton, NJ
Lumbar Fusion

Rodney Harraway
Wilkes Barre, PA
Lumbar Fusion

Marlene Socarras
Long Island City, NY
Lumbar Fusion

Kathy Trenholm
Washington, DC
Lumbar Fusion
Daniel Sapen
Huntington Station, NY
Lumbar Fusion
Cathleen Malden
Valley Cottage, NY
Lumbar Fusion

Joan Duncan
Norwalk, CT
Lumbar Fusion

Richard Torvinen
Bristol, CT
Lumbar Fusion

Christopher Cardinoza
North Brunswick, NJ
Lumbar Fusion

Barbara Miller
Orange, CT
Lumbar Fusion
References
- Adl Amini D, Moser M, Oezel L, Shue J, Pumberger M, Sama AA, Cammisa FP, Girardi FP, Hughes AP. Fusion assessment in standalone lateral lumbar interbody fusion: 3D-printed titanium versus polyetheretherketone (PEEK) cages. J Spine Surg. 2022 Sep;8(3):323-332. doi: 10.21037/jss-22-17. PMID: 36285103; PMCID: PMC9547697. https://pubmed.ncbi.nlm.nih.gov/36285103/
- Alluri R, Mok JK, Vaishnav A, Shelby T, Sivaganesan A, Hah R, Qureshi SA. Intraoperative Neuromonitoring During Lateral Lumbar Interbody Fusion. Neurospine. 2021 Sep;18(3):430-436. doi: 10.14245/ns.2142440.220. Epub 2021 Sep 30. PMID: 34610671; PMCID: PMC8497239. https://pubmed.ncbi.nlm.nih.gov/34610671/
- Derman PB, Albert TJ. Interbody Fusion Techniques in the Surgical Management of Degenerative Lumbar Spondylolisthesis. Curr Rev Musculoskelet Med. 2017 Dec;10(4):530-538. doi: 10.1007/s12178-017-9443-2. PMID: 29076042; PMCID: PMC5685965. https://pubmed.ncbi.nlm.nih.gov/29076042/
- Manzur M, Virk SS, Jivanelli B, Vaishnav AS, McAnany SJ, Albert TJ, Iyer S, Gang CH, Qureshi S. The rate of fusion for stand-alone anterior lumbar interbody fusion: a systematic review. Spine J. 2019 Jul;19(7):1294-1301. doi: 10.1016/j.spinee.2019.03.001. Epub 2019 Mar 11. PMID: 30872148. https://pubmed.ncbi.nlm.nih.gov/30872148/
- Manzur MK, Steinhaus ME, Virk SS, Jivanelli B, Vaishnav AS, McAnany SJ, Albert TJ, Iyer S, Gang CH, Qureshi SA. Fusion rate for stand-alone lateral lumbar interbody fusion: a systematic review. Spine J. 2020 Nov;20(11):1816-1825. doi: 10.1016/j.spinee.2020.06.006. Epub 2020 Jun 11. PMID: 32535072. https://pubmed.ncbi.nlm.nih.gov/32535072/
- Pawar A, Hughes A, Girardi F, Sama A, Lebl D, Cammisa F. Lateral Lumbar Interbody Fusion. Asian Spine J. 2015 Dec;9(6):978-83. doi: 10.4184/asj.2015.9.6.978. Epub 2015 Dec 8. PMID: 26713134; PMCID: PMC4686408. https://pubmed.ncbi.nlm.nih.gov/26713134/
- Salzmann SN, Fantini GA, Okano I, Sama AA, Hughes AP, Girardi FP. Mini-Open Access for Lateral Lumbar Interbody Fusion: Indications, Technique, and Outcomes. JBJS Essent Surg Tech. 2019 Nov 1;9(4):e37.1-10. doi: 10.2106/JBJS.ST.19.00013. PMID: 32051785; PMCID: PMC6974316. https://pubmed.ncbi.nlm.nih.gov/32051785/
- Salzmann SN, Shue J, Hughes AP. Lateral Lumbar Interbody Fusion-Outcomes and Complications. Curr Rev Musculoskelet Med. 2017 Dec;10(4):539-546. doi: 10.1007/s12178-017-9444-1. PMID: 29038952; PMCID: PMC5685966. https://pubmed.ncbi.nlm.nih.gov/29038952/
- Shahi P, Vaishnav A, Araghi K, Shinn D, Song J, Dalal S, Melissaridou D, Mai E, Dupont M, Sheha E, Dowdell J, Iyer S, Qureshi SA. Robotics Reduces Radiation Exposure in Minimally Invasive Lumbar Fusion Compared With Navigation. Spine (Phila Pa 1976). 2022 Sep 15;47(18):1279-1286. doi: 10.1097/BRS.0000000000004381. Epub 2022 Jun 29. PMID: 35791068. https://pubmed.ncbi.nlm.nih.gov/36285103/
- Sivaganesan A, Kim C, Kiran Alluri R, Vaishnav AS, Qureshi S. Advanced Technologies for Outpatient Lumbar Fusion: Barriers and Opportunities. Int J Spine Surg. 2022 Oct;16(S2):S37-S43. doi: 10.14444/8275. Epub 2022 Jul 13. PMID: 35831061; PMCID: PMC9808792. https://pubmed.ncbi.nlm.nih.gov/35831061/
- Subramanian T, Araghi K, Sivaganesan A, Shahi P, Vaishnav A, Iyer S, Qureshi SA. Ambulatory Lumbar Fusion: A Systematic Review of Perioperative Protocols, Patient Selection Criteria, and Outcomes. Spine (Phila Pa 1976). 2023 Feb 15;48(4):278-287. doi: 10.1097/BRS.0000000000004519. Epub 2022 Nov 4. PMID: 36692157. https://pubmed.ncbi.nlm.nih.gov/36692157/
- Swiatek PR, McCarthy MH, Weiner J, Bhargava S, Vaishnav AS, Iyer S. Intraoperative image guidance for lateral position surgery. Ann Transl Med. 2021 Jan;9(1):90. doi: 10.21037/atm-2020-ioi-10. PMID: 33553383; PMCID: PMC7859765. https://pubmed.ncbi.nlm.nih.gov/33553383/
- Weiner JA, McCarthy MH, Swiatek P, Louie PK, Qureshi SA. Narrative review of intraoperative image guidance for transforaminal lumbar interbody fusion. Ann Transl Med. 2021 Jan;9(1):89. doi: 10.21037/atm-20-1971. PMID: 33553382; PMCID: PMC7859762. https://pubmed.ncbi.nlm.nih.gov/33553382/