How to Correct Bowlegs in Adults
Bowlegs, also sometimes called “bow legs” or “bowed legs,” is a common condition where the knees don’t come together when the feet are touching. The medical term for bowlegs is genu varum. This article focuses on bowlegs in adults, including teenagers who have reached skeletal maturity (completed growth). It answers some common questions people ask about this condition and describes the different surgical treatments available.

Are bowlegs painful?
People with bowlegs often complain of knee or ankle discomfort and they worry about the development of future arthritis. Many young people have little pain but are self-conscious about the appearance of their legs and do not even realize the danger that lies ahead for many of them. In middle aged people, bowlegs are associated with degeneration of the inside of the knee, which is often quite painful.
Why should I correct my bowlegs?
Damage may be occurring to your knee: With bowing, the knee experiences unbalanced loads that it was not designed to handle. This leads to excessive stress, resulting in tearing of the medial meniscus and articular cartilage and can cause IT band pain. In the joint the cartilage fissures and delaminates until bone starts rubbing against bone. Several factors accelerate the decline of the knee joint: obesity, a family history of arthritis, and high physical activity. In other words, both overweight and fit people with bowlegs are at risk!
Abnormal foot rotation torques the knee: Many people who have bowlegs also have mal-rotation, or torsion, of the tibia. This means that either the feet turn inward or outward as compared to the knees. A review of patients that have come to our service for bowleg correction half have had rotational malalignment. The torsion may be obvious if the feet turn outward while walking. However, many times the rotational component is subtle. For example, patients with external tibial torsion will walk with the feet straight and the knees squinting inward.

Photo showing outward turning of the feet, indicating tibial torsion.

Photo showing "squinting" knees when feet are facing forward.
This is most obvious when these people run and their feet and legs are self-described as “looking like a helicopter.” They may have difficulty riding a bicycle as the knees can knock against the bike frame. This torsion twists the knee joint (and the ankle joint), and over time causes shear injury to the meniscus and joint cartilage.
Can bowlegs be corrected without surgery?
The belief that bowlegs can be corrected without surgery is a fallacy. Varus deformity around the knee is a structural deviation from normal bone alignment. Exercise, stretching, strengthening, physical therapy, and vitamins will make your muscles and bones stronger but will not change the shape of the bones. The only way to truly change the shape of the legs is to cut the bone and straighten it. This is called an osteotomy and is an enduring, structural alteration.
Restoring proper bone structure will improve function: Proper limb alignment affects the entire body in a positive way. The muscles and tendons are pulling along their intended trajectory, optimizing their efficiency. The ligaments, which hold the joints together, no longer experience undue stress. High-performance athletes who came to me with bowleg-related knee pain were able to return to sports at a higher level of function and performance after surgery. The best results can be expected in cases where the knee is not already burdened with arthritis.
Correcting bowlegs may avert the need for future surgery. For example, many people with uncorrected bowlegs may have to have knee replacement in their future and earlier in life than typical candidates for knee replacement. Although a total knee replacement can provide a good result, it is certainly not as optimal as saving the native knee. An osteotomy surgery to correct the bowing may be the antidote to avoid knee replacement.
In the twenty-first century, patients have become well-informed and take ownership of their healthcare. The internet has helped educate patients about surgeries and medical specialists that might not have existed 20 or 30 years ago. This exposure to different surgical techniques has led patients to consider which may be the best fit for them.
The various surgeries available to correct bowlegs are great examples. There are many different surgical options to arrive at the same result. Although these different procedures may seem interchangeable, there are often patient-specific anatomic features that will dictate the need for one procedure over another in a particular individual.
What are the surgical treatments to correct bowlegs?
There are various surgical methods, appropriate for different people depending on their specific bowleg condition. All involve an osteotomy (cutting and reshaping the bone) of either the tibia (shinbone), the femur (thighbone), or both. These are known as tibial osteotomies and distal femoral osteotomies. Bowleg corrective surgical methods include:
- tibial and/or distal femoral osteotomy with internal fixation of plate and screws
- tibial osteotomy with an intramedullary nail
- tibial osteotomy with gradual correction using circular external fixation
Tibial osteotomy with an internal plate and screws
This is my preferred method for correcting a simple bowleg deformity. It is appropriate only when:
- The varus, or bowing, is occurring in the tibia bone (a opposed to the femur).
- The deformity is less than 12 degrees.
- There is no rotational deformity, and that the bone is of normal density (meaning the patient does not have osteoporosis).
Although these criteria are somewhat restrictive, people who undergo this procedure are quite comfortable. The surgery is minimally invasive and the plate is small. Partial weightbearing is allowed immediately after surgery. The recovery is simple and nearly painless.

Before and after X-rays of tibial osteotomy surgery with internal fixation using plates and screws.
Distal femoral osteotomy (DFO) with internal fixation
In some cases, the femur will be selected as the optimal site for the bowleg correction. This occurs in large bowing deformities where there is greater than 12 degrees of varus. Both the femur and tibia will be realigned yielding an optimal result. The femoral osteotomy is also stabilized with a plate and screws. Femoral osteotomy may be preferred in older patients where healing can be expected to be faster and immediate weight-bearing allowed.
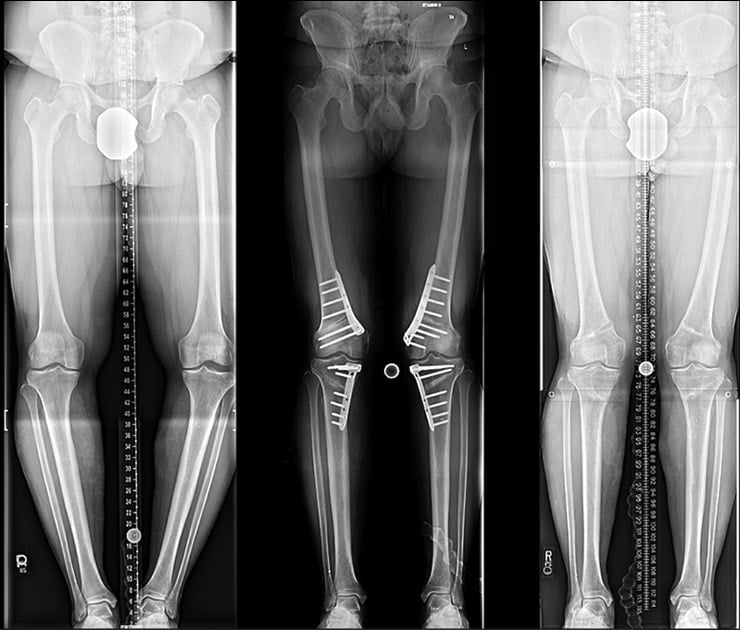
Before and after X-rays of bowleg correction using a DFO and tibial osteotomy with internal fixation.
Tibial osteotomy with intramedullary (IM) nailing
In patients with both rotational deformity and varus of the tibia, IM nails can be used to offer an all-internal solution to this complex problem. Improvements in surgical instrumentation and intra operative alignment measurement tools have made this method accurate and reproducible. The method involves creating an osteotomy and then inserting a titanium rod down the hollow bore of the tibia. Screws are used to fix the bones in the ideal position. This method is technical and not appropriate for large bowleg deformities.
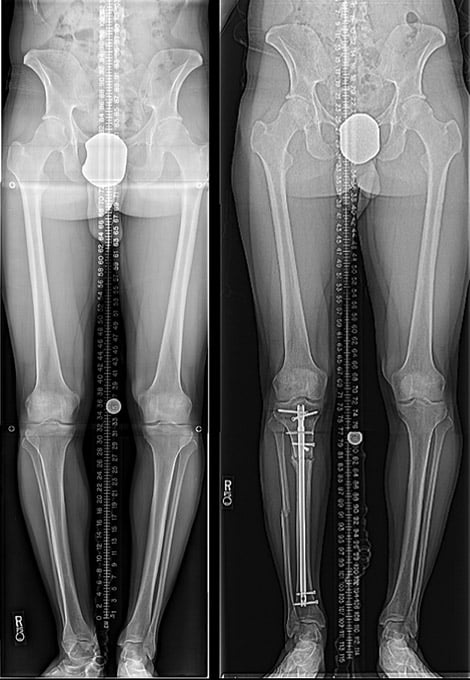
Before and after X-rays of a person with bowleg and rotational deformity having a tibial osteotomy with intramedullary nailing.
Circular external fixation
Circular frames, or those that use rings, are versatile and powerful tools for deformity correction. They can correct many deformities simultaneously. So, patients who have severe bowing in the tibia only (tibia varus greater than 10 to 12 degrees) or who have associated tibial torsion, a loss of knee extension, or a leg length discrepancy can have all of these malalignments fixed simultaneously. Patients may walk right after surgery and adjust the frame while at home. Follow-up is critical and can be done virtually or in person. The bone is straightened gradually, which is excellent for healing, and it is exciting for the patient to see their leg growing straighter. New advances in external fixation have delivered automatic, self-adjusting struts making the process even easier. Once the correction is complete, the external fixation is removed.

Before and after X-rays of a person with large bowleg deformity who had surgery with circular external fixation.
Conclusion
These three different approaches to correcting bowlegs are tailored to the exact needs of the patient as dictated by the bony deformity and the physical examination. Although a patient may desire a certain method of surgery, a comprehensive exam and radiographs will direct optimal treatment.
