Correction of Severe Congenital Scoliosis in a 28-Year-Old Man
From Grand Rounds from HSS: Management of Complex Cases | Volume 12, Issue 2
Case Report
A 28-year-old man presented with early-onset scoliosis resulting in 20 years of debilitating back pain and spasms. He wore a brace for the first 5 years of his life but then stopped. Of note, his brothers were 6’ tall, while he was 5’3”, presumably secondary to the spinal deformity.
Examination found a significant rib rotation in the chest, causing the left posterior chest wall to protrude posteriorly. His neurologic strength was 5/5 in all major muscle groups, and he did not have hyperreflexia.
Scoliosis films showed a 135° apex left thoracic Cobb angle with a 75° thoracic kyphosis (Fig. 1). Magnetic resonance imaging (MRI) of the cervical, thoracic, and lumbar spine did not show notable spinal stenosis or spinal cord anomalies. Pulmonary function testing showed significant restrictive lung disease.
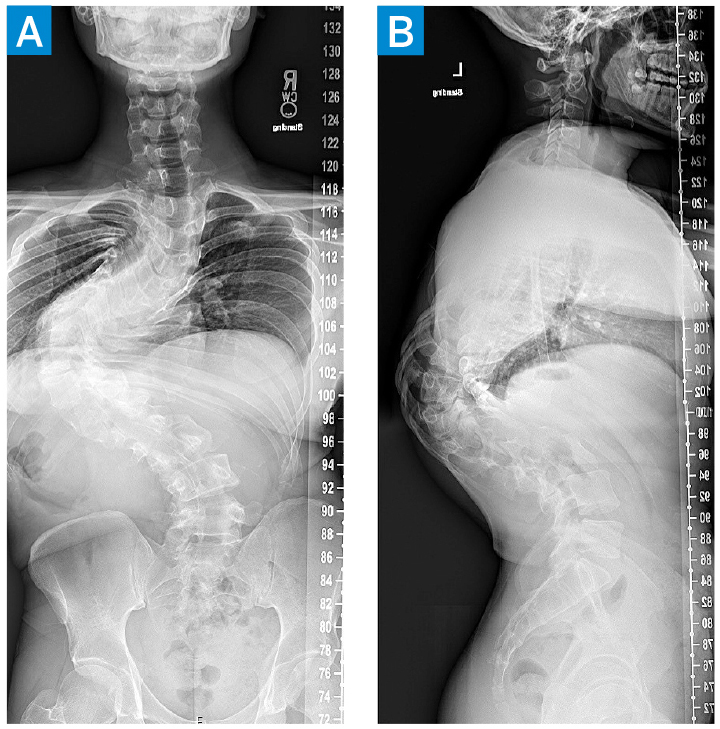
Figure 1: Posteroanterior (A) and lateral (B) scoliosis radiographs show a 135° apex left thoracic curve with a 75° thoracic kyphosis.
The patient underwent a T2–L4 posterior segmental instrumented fusion with posterior column, or Ponte, osteotomies at T6–L1. The Ponte osteotomies helped to improve the flexibility of the spine, but despite this “softening” of the curve’s apex, it remained relatively stiff, suggesting that translation of the apex toward midline for the correction would be a challenge. Intraoperative 3D fluoroscopy showed significant vertebral body rotation and dysplastic pedicles, particularly near the T8–T11 apex (Fig. 2), which would make challenging the placement of screws at the apex of the curve using standard “freehand” methods and with risk for neurological injury.
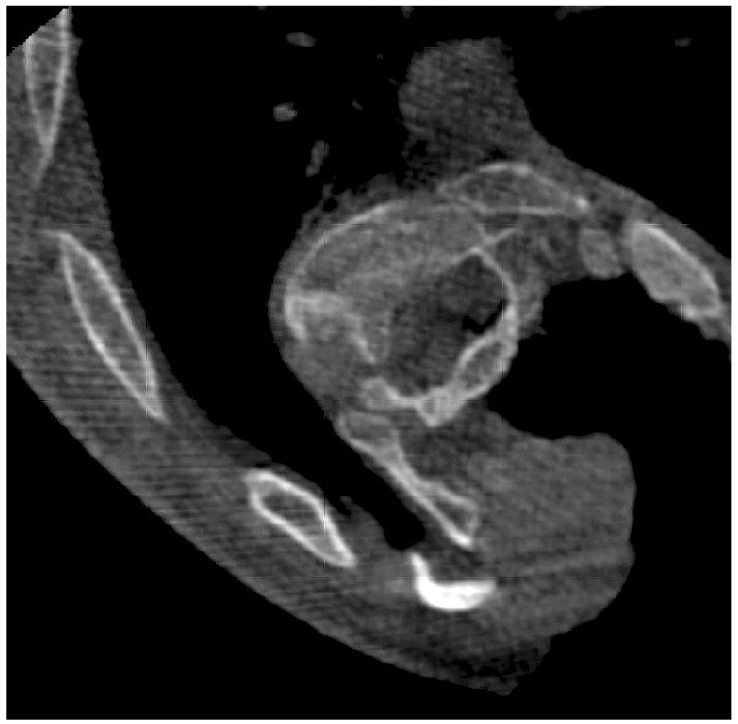
Figure 2: Intraoperative 3D fluoroscopy shows 90° rotation of the vertebral body with dysplastic pedicles.
We employed hook and screw fixation proximally and pedicle screws distally using freehand methods, sublaminar wires to help with apex translation, and computer-assisted 3D navigation to place the screws in the apex of the deformity, with constant neuromonitoring feedback. The rods selected had the stiffness needed to withstand the forces required for correction. A femoral distractor was anchored to 3 proximal thoracic and the 3 distal lumbar instrumented levels on the right side; it was used to gradually lengthen and mobilize the spine while the wires were sequentially tightened to translate the spine toward the midline from their connection point on the right rod. As the spine was reduced toward the right rod, a left rod was placed, and a combination of derotational, cantilever, and compression/distraction techniques was used to complete the correction.
Postoperatively, the patient was hospitalized for 7 days and remained neurologically intact. He developed ileus that rapidly resolved after placement of a nasogastric tube; he mentioned discomfort in the rectus and anterior oblique muscles that resolved within 2 weeks and mild-to-moderate neuropathic pain in the legs that resolved by the 6-week follow-up. At 4-year follow-up, he maintained more than 50% correction to a 60° thoracic Cobb angle and a 25° thoracic kyphosis (Fig. 3). He gained nearly 6” in height and is now 5’9” tall.
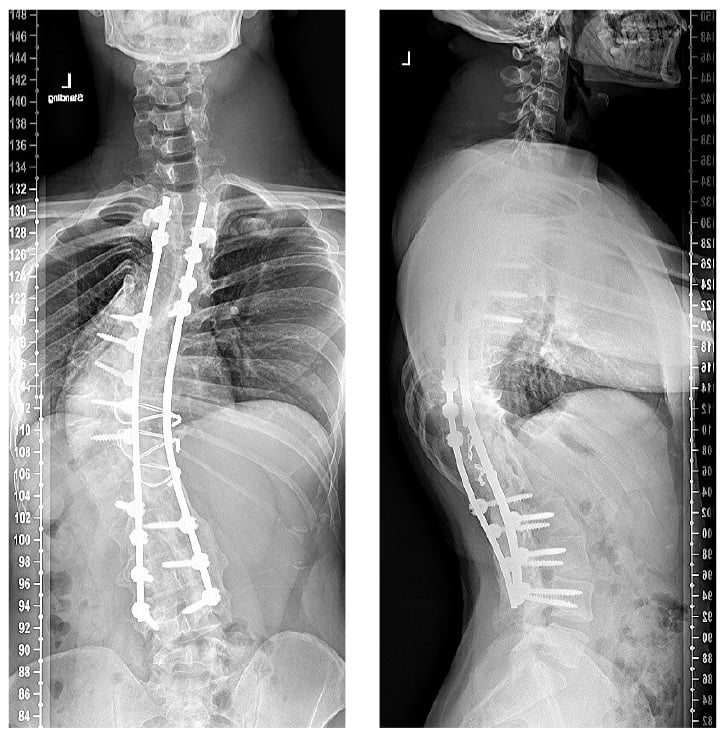
Figure 3: At 4-year follow-up after T2–L4 posterior segmental instrumented fusion, the patient showed a greater than 50% correction to a 60° thoracic Cobb angle and a 25° thoracic kyphosis.
Discussion
Severe spinal deformity presents challenges to surgeons: pedicle screw placement may not be accomplished under freehand or fluoroscopic guidance, and severely dysplastic pedicles may require replacement of pedicle screws with sublaminar wiring or hooks [1]. Unfortunately, such techniques do not allow the corrective strength that pedicle screw fixation does [2]. Pedicles are also most dysplastic at the apex of the curve and raise the risk for spinal cord injury if screws are breeched medially [3]. Given the degree of rotation and pedicle dysplasia in this case, computer assisted navigation allowed the safe placement of multiple screws in the apex of the curve to maximize the surgical reduction.
The use of preoperative traction in the treatment of severe spinal deformity is controversial. Gradual sustained correction through traction can maximize final deformity correction, but studies at HSS found that halo traction resulted in a 30% complication rate without necessarily improving correction [4,5], while also posing a significant burden to the patient and caretaker. Various intraoperative traction methods used to supplement correction of large curves with good results included intraoperative halo traction, femoral traction, and rib and hip distractors [6,7]. We opted for intraoperative traction using a femoral distractor mounted on the pedicle screws to provide gradual correction without extending outside of the surgical field, in addition to acute correction through rod contouring. Distraction through pedicle screws risks plow through, but we obtained good purchase through the use of navigated pedicle screw placement.
Authors

References
- Suk SI, Lee CK, Min HJ, Cho KH, Oh JH. Comparison of Cotrel-Dubousset pedicle screws and hooks in the treatment of idiopathic scoliosis. Int Orthop. 1994;18(6):341-346. doi:10.1007/BF00187077.
- Esposito VR, Dial BL, Fitch RD, Lark RK. Periapical wires result in less curve correction than pedicle screw constructs in idiopathic scoliosis. Asian Spine J. 2019;13(6):1010-1016. doi:10.31616/ asj.2019.0001.
- Wang S, Qiu Y, Liu W, et al. The potential risk of spinal cord injury from pedicle screw at the apex of adolescent idiopathic thoracic scoliosis: magnetic resonance imaging evaluation. BMC Musculoskelet Disord. 2015;16:310. doi:10.1186/s12891-015-0766-0.
- Iyer S, Duah HO, Wulff I, et al. The Use of halo gravity traction in the treatment of severe early onset spinal deformity. Spine (Phila Pa 1976). 2019;44(14):E841-E845. doi:10.1097/ BRS.0000000000002997.
- Sponseller PD, Takenaga RK, Newton P, et al. The use of traction in the treatment of severe spinal deformity. Spine (Phila Pa 1976). 2008;33(21):2305- 2309. doi:10.1097/BRS.0b013e318184ef79.
- Bachman DR, Singh LK, Anderson JT, Schwend RM. An intraoperative laterally placed distractor for gradual load sharing correction of severe spastic Case 3 Continued neuromuscular spinal deformity. Spine Deform. 2021;9(4):1137-1144. doi:10.1007/s43390-021- 00316-4.
- Jackson TJ, Yaszay B, Pahys JM, et al. Intraoperative traction may be a viable alternative to anterior surgery in cerebral palsy scoliosis ≥100 degrees. J Pediatr Orthop. 2018;38(5):e278-e284. doi:10.1097/BPO.0000000000001151.