Oncologic Allograft Femur Nonunion Treated with the Internal Lengthening and Compression Nail
From Grand Rounds from HSS: Management of Complex Cases | Volume 11, Issue 2
Case Report
A 54-year-old man diagnosed with osteosarcoma 17 years prior to presentation had undergone tumor resection with intercalary allograft placement and postoperative chemotherapy. A year later an implant fracture was complicated by infection with a resistant strain of Staphylococcus aureus. Several years later, a femoral allograft fracture required partial graft excision and placement of an intramedullary nail. The fracture failed to unite, leading to further implant fracture and loss of fixation.
When the patient presented to HSS, the nail had migrated distally through the intercondylar fossa, resulting in knee pain and loss of extension. A 10-cm leg length discrepancy made ambulation difficult (Fig. 1); a recalcitrant femur nonunion found on physical examination was possibly complicated by residual infection in the allograft bone and implant fragments in the femur.
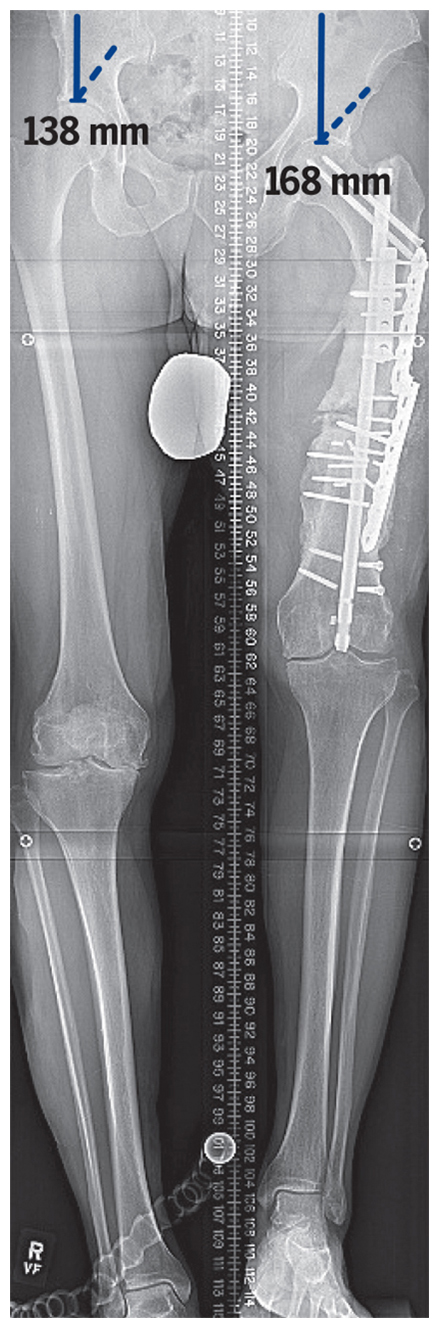
Figure 1: Standing radiograph shows 10 cm leg length discrepancy and numerous retained implants.
A complex reconstruction was planned, divided into stages. First, we removed the retained hardware and performed a meticulous debridement of dead bone and allograft. We eliminated approximately 1 inch of dead space by using a PRECICE® nail to provide compression. Fortunately, preoperative laboratory workup, intraoperative assessment, and operative cultures were negative for infection. Some of the enveloped allograft provided structure and was retained. There was extensive new vascularized bone growth around the allograft, and given the femur shortening, native bone union could be achieved by strongly compressing the femur for a prolonged period using the PRECICE nail (Fig. 2).
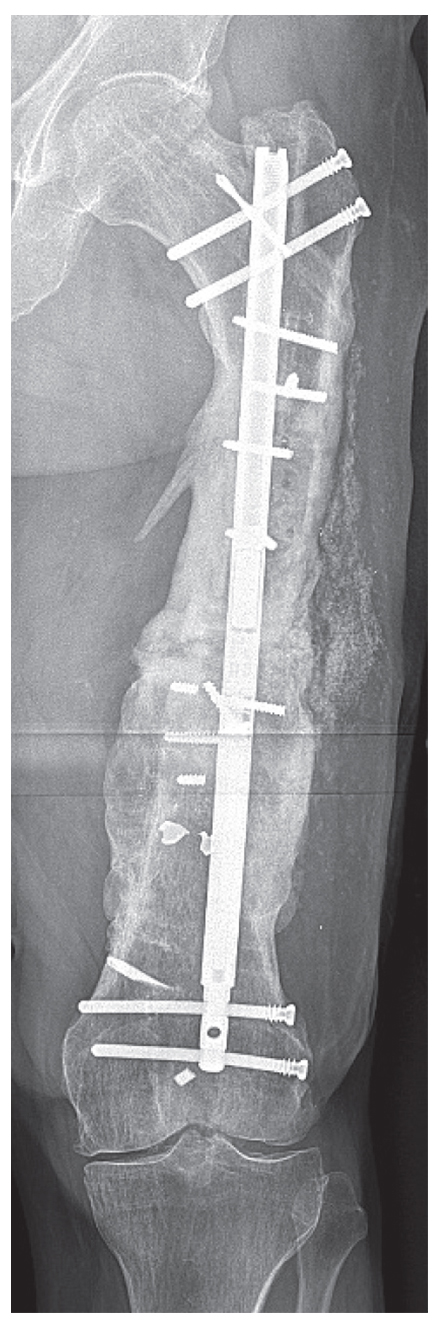
Figure 2: Anteroposterior radiograph of the femur shows healing of the nonunion following compression with the nail. Note bending of the locking screws.
Next, we performed a staged lengthening in the femur and tibia. The antegrade femur nail was exchanged for a retrograde PRECICE nail because the distal osteoplasty site provided the best regenerative potential. The patient also had overall varus alignment of the extremity; we placed a temporary external fixator in the tibia to perform an acute correction into valgus through the osteoplasty site, which would be maintained by blocking screws placed around the PRECICE nail (Fig. 3). Following distraction and consolidation of the femur and tibia, the leg lengths were equalized and the implants removed (Fig. 4). At 1.5-year follow-up, the patient had no pain in the left knee but subsequently underwent contralateral total knee arthroplasty for varus osteoarthritis.
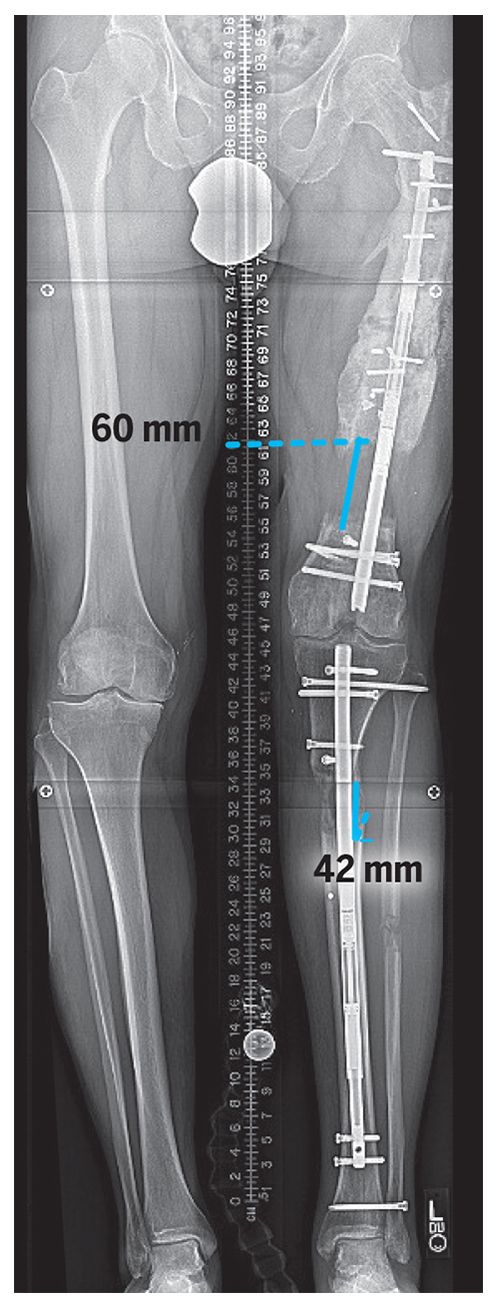
Figure 3: Standing radiograph at the end of distraction of the femur and tibia. Note blocking screws in the femur and tibia.

Figure 4: Standing radiograph following femur and tibia regenerate consolidation and removal of the lengthening nails.
Discussion
This case illustrates the challenges of femoral nonunion when surrounding soft tissues and vascularity have been traumatized by cancer resection and subsequent surgeries. Biological stimulus such as bone morphogenetic protein cannot be used in patients with a history of cancer due to the potential for tumor recurrence, although mechanical means such as sustained compression can be used. Compression nailing, a magnetic lengthening nail used in reverse, provides a powerful means of healing long bone nonunion [1, 2]. Compression of the nonunion will produce deflection of the locking screws, which provides feedback that the nonunion site is still under a compressive load. Loss of the screw bending should be noted and treated with further compression. Sacrificing a small amount of bone length to obtain more circumferential surface area for bone union is acceptable and was done in this case.
Simultaneous lengthening of tibia and femur can more quickly resolve a large leg length discrepancy [3, 4]. Our patient’s femur was so traumatized and its regenerative potential so poor it would be imprudent to expect a 10-cm lengthening without contribution from the tibia. When lengthening the femur and tibia simultaneously, the overall change in length of the extremity should be considered and not exceed 1–1.2 mm/day, so that each distraction index is lower (~0.4–0.6 mm/day) than is typical. When lengthening at osteoplasty sites, the surgeon should choose bone areas with preserved vascularity if possible; we chose a distal site, away from the prior open surgery/nonunion in the femur, and used a very slow rate of distraction to produce a quality regenerate. Even so, our patient required an instillation of bone marrow from the iliac crest to achieve healing.
Finally, blocking screws placed around lengthening nails are useful during both nail insertion (to direct the path of the reamers/nail) and lengthening (to prevent implant migration and creation of deformity). We used them in both the femur and the tibia in this case. Uneven knee height is expected when lengthening the femur and tibia to treat femur shortening, but anecdotal evidence has shown a knee height discrepancy of up to 5 cm may be tolerated, as it was in this patient.
Authors

Attending Orthopedic Surgeon, Hospital for Special Surgery
Assistant Professor of Orthopedic Surgery, Weill Cornell Medical College

Attending Orthopedic Surgeon, Hospital for Special Surgery
Director, Limb Salvage and Amputation Reconstruction Center, Hospital for Special Surgery
References
- Fragomen AT. Transitioning to an intramedullary lengthening and compression nail. J Orthop Trauma. 2017;31 Suppl 2:S7-S13. doi:10.1097/BOT.0000000000000842.
- Fragomen AT, Wellman D, Rozbruch SR. The PRECICE magnetic IM compression nail for long bone nonunions: A preliminary report. Arch Orthop Trauma Surg. 2019;139(11):1551-1560. doi:10.1007/s00402-019-03225-4.
- Kirane YM, Fragomen AT, Rozbruch SR. Precision of the PRECICE internal bone lengthening nail. Clin Orthop Relat Res. 2014;472(12):3869-3878. doi:10.1007/s11999-014-3575-0.
- Sheridan GA, Falk DP, Fragomen AT, Rozbruch SR. Motorized internal limb-lengthening (MILL) techniques are superior to alternative limb-lengthening techniques: A systematic review and meta-analysis of the literature. JBJS Open Access. 2020;5(4):e20.00115. doi:10.2106/JBJS.OA.20.00115.