Ankle Instability: Causes, Diagnosis and Treatment
Every day an estimated one out of every 10,000 people sprain their ankle, an injury in which one of the two major ligaments on the outer portion of the ankle is stretched and/or torn. (As shown below, these are the anterior talofibular ligament and the calcaneofibular ligament.)
In the great majority of cases, individuals who see a physician for their injury are instructed on how to reduce pain and inflammation. They may be advised to wear an air cast or participate in physical therapy to strengthen the ankle muscles, in order to make a full recovery. The remaining population – about 10% of people – develop ankle instability,
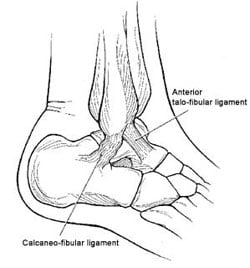
Line drawing of the anatomy of the lateral or outer ankle with the two major ligaments.
What is ankle instability?
Ankle instability is a condition in which the ligament from a sprained ankle has healed but in a lengthened position. As a result, the person is prone to a feeling of the ankle "giving out" and to experiencing further sprains. Athletes such as ballet dancers, who already have looser-than-average ligaments, are particularly likely to develop this condition.
How is ankle instability diagnosed?
The orthopaedic surgeon diagnoses ankle instability through a physical assessment for mechanical instability (motion beyond the normal physiological range) and through the use of taler tilt (or stress) X-rays. In a healthy ankle, this tilt should only extend to about 5°. In the patient with an unstable ankle, the tilt will extend to 15° to 20° on X-ray.
How is ankle instability treated?
Treatment for ankle instability begins with a regimen of exercises intended to strengthen the muscles of the outer ankle, in an attempt to compensate for the loss of stability formerly provided by the ligament. While this treatment is helpful for many patients, it may be less successful in individuals whose muscles are already quite strong, such as dancers or other athletes.
If instability is primarily a problem when participating in specific recreational activities, it may be addressed by taping the ankle and/or with the use of a brace, either one that is worn in an athletic shoe, or one that laces around the ankle. However, if these measures are not adequate to restore stability and the patient continues to experience a feeling of instability during everyday activities, surgical repair of the injury may be advised.
What is the surgery for ankle instability?
There are two types of surgical intervention. The preferable option is an anatomic ligament reconstruction. The second type is a peroneal substitution ligament reconstruction, where the ligament is replaced a tendon from the patient’s ankle.
Anatomic reconstruction
This is the preferred method. Here, the stretched or torn ligaments is repaired and allowed to heal in a shorten position. This reconstruction can be accomplished by using the patient’s own tissue, also known as a Broström procedure, or utilize a cadaver tendon, also called an allograft, if the patient’s own tissue is too stretched out or different. For added stability and to help prevent re-injury, the surgeon may also tighten the retinaculum, a band of fibrous tissue that helps hold the ankle in proper alignment.
In almost all cases, anatomic reconstruction is possible and preferable. This procedure offers the advantages of maintaining full mobility of the joint, a smaller incision, and a more rapid recovery. The primary drawback of this procedure is that ligaments may become loose a second time and require additional repairs, but this is rare. Results of the Broström procedure performed at HSS are excellent. In a case series of seventy-three patients, all but one was satisfied with the procedure and would have the procedure again.
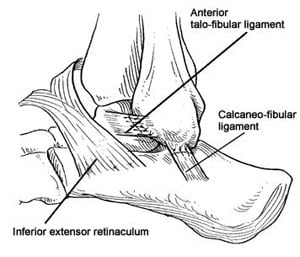
Anatomic reconstruction.
However, anatomic reconstruction, using a patient’s own tissue, is not possible in every case, for example, when the tissue have been too damaged and are insufficient for repair. When the torn ligament is too badly damaged we utilize a tendon allograft.
Peroneal substitution ligament reconstruction
In this procedure, the ligament is replaced entirely with a piece of tendon from the patient’s ankle. This procedure is less ideal because the peroneal tendon, which is the main dynamic stabilizer of the ankle, is used to harvest tha graft for the new ligament.
Peroneal substitution ligament reconstruction requires a larger incision than anatomic reconstruction, has a somewhat longer recovery period, and carries a risk of nerve irritation, which can lead to chronic pain. We rarely use a non-anatomic personal substitution ligament reconstruction because it sacrifices a good tendon, has higher instances of post-operative stiffness and pain.
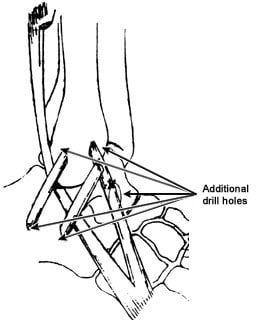
Peroneal Substitution
What kind of anesthesia is used for ankle instabilty surgery?
Regardless of which type of orhopedic procedure is performed, at HSS, it will be done using an epidural – the same type of anesthesia that many women receive during childbirth – so that the patient may be awake during their surgery if they so choose. Surgery for ankle instability is an outpatient surgery. An overnight stay in the hospital is not necessary.
How successful is ankle instabilty surgery?
Long-term outcome for both of these surgical procedures is generally quite good, provided that there is no arthritis present in the ankle. Ankle instability is not necessarily associated with ankle arthritis. However, if the bones of the ankle have been rubbing against each other over the course of many years owing to chronic ankle instability, then the latter condition may contribute to the wearing away of cartilage, and the development of arthritis in the joint.
What is the recovery time for ankle instability surgery?
Following surgery, the ankle is placed in a plaster splint and the patient must use crutches or a knee scooter to avoid placing any weight on the affected foot. At two weeks, the plaster splint is replaced with a cast or removable boot, which is worn for an additional 2 to 4 weeks. Formal physical therapy is started at 6 weeks and an ankle support is worn for walking until 12 weeks after surgery. By 10 to 12 weeks, most people no longer require a brace and can return to all their normal activities including participation in sports.
At HSS, orthopedic surgeons also treat patients who require a second surgery after anatomic reconstruction, because the ligaments have once again become too loose. In these cases, replacement with a tendon may be advised. Individuals who have undergone ankle ligament reconstruction may also seek treatment if they are experiencing pain due to nerve irritation or ankle stiffness. These situations can be very difficult and should be treated by an experienced foot and ankle surgeon.
