Hip Preservation Service
Leaders in the research, diagnosis and treatment of hip disorders
The hips are critical to our body’s mobility and stability. If a hip disorder is not diagnosed and left untreated, it can lead to hip disease and serious degeneration. Research shows that early intervention techniques like hip arthroscopy and periacetabular osteotomy (PAO) could delay or prevent painful arthritis that leads to hip replacement surgery.
The Hip Preservation Service at HSS specializes in the broad range of hip conditions like femoral acetabular impingement (FAI), hip dysplasia and labral tears that can occur at any stage of life, from young children to teens, active adults and seniors. Our hip joint specialists are innovative leaders from various specialties working in a collaborative, multidisciplinary environment to provide the highest level of care.

I am thankful every day to compete and simply walk without pain. - Lauren, HSS patient
Our goal is to relieve hip pain and preserve the joint
While surgery is always the last resort, our surgeons are the best at what they do. We employ the following techniques to bring the best possible results to our patients:
- The latest minimally invasive surgical techniques for a faster recovery and to reduce the need for more extensive surgeries.
- Joint-preserving treatment options for young, active adult patients suffering from hip pain to restore a high level of function.
- Advanced imaging and testing to determine early hip disease, achieve an accurate diagnosis, and recommend proper treatment.
- Our leading scientists and clinicians can identify various stages of hip disease and dig deeper into their underlying causes.
What Causes Hip Pain
The joints, bones, muscles and ligaments of the hip and pelvic areas are intricately balanced but can be vulnerable to wear and tear. Many factors can cause hip pain or hip problems that would lead someone to seek medical treatment from an orthopedist. These include:
- abnormal anatomy that a person is born with and conditions that develop during the growth and development of the bones grow in childhood or adolescence
- trauma, as well as the wear and tear that occurs with aging can all lead to progressive arthritic changes
- hip pain in athletes is commonly the result of a muscle strain or tendinitis
The diagnosis and management of hip injuries has evolved substantially with the advancement in diagnostic tools such as magnetic resonance imaging and with new minimally invasive techniques and in hip arthroscopy.
Hip labral tears: What they are and how to treat them
Watch a panel with three hip preservation surgeons and a physiatrist discuss labral tears and how to determine if surgery is needed.
The anatomy of the hip joint
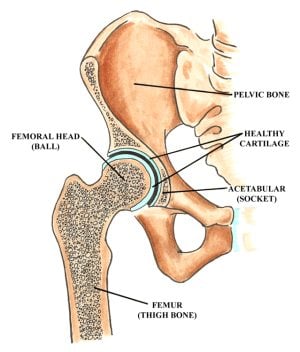
The hip joint is a “ball and socket” joint located where the thigh bone (femur) meets the pelvic bone. The upper segment (“head”) of the femur is a round ball that fits inside the cavity in the pelvic bone that forms the socket, also known as the acetabulum. The ends of the bone are covered with a smooth, cushioning layer called articular cartilage. The articular cartilage is what allows the bones to glide smoothly. While the cartilage covers the entire head of the femur, the acetabulum cartilage is in the shape of a horseshoe with a depression (fossa) in the center of the socket. This fossa contains soft tissue and a ligament connecting the femoral head to the socket.
The socket has a rim of rubbery fibrocartilage called the labrum. The labrum acts as a gasket, sealing in joint fluid and maintaining lubrication and nutrition. In addition, numerous tendons surround the hip, as well as bursae, which are lubrication "cushions" where soft tissues glide over bony prominences.
Our team of medical specialists is committed to joint-preserving treatment options for the hip. They are knowledgeable in a range of treatment options from the nonsurgical to the most complex. Our comprehensive team approach utilizes experts in the fields of orthopedics, radiology, physiatry, sports medicine, physical therapy, rheumatology, and bio-engineering. Working hand-in-hand with our researchers, our staff is constantly evaluating and improving our surgical techniques and investigating new approaches.
Our Team
















Personalized Patient Care
Using a multi-disciplined approach to the understanding of hip pain and treatment, the Service combines the expertise of a wide variety of health care professionals including orthopedic surgeons, radiologists, physiatrists, physical therapists, and a multitude of musculoskeletal experts and clinical researchers so patients can benefit from a coordinated treatment experience.
Comprehensive Treatment
Through years of experience and research, our specialists have been able to better identify underlying conditions in earlier stages, providing patients with more treatment options that help to preserve the integrity of the hip joint, including nonsurgical options and minimally invasive arthroscopic surgical techniques.
- Learn more about treatment options to preserve the hip joint.
- See how physical therapy and rehabilitation plays an integral role in every step of the treatment.
More Patient Resources
- Activities and Exercises to Strengthen your Hips
- Frequently Asked Questions - answers to commonly asked questions
- Related Services - HSS has a wealth of departments that work together to bring you the best orthopedic care in the US.
- View our periacetabular osteotomy (PAO) animation - Narration is included so please remember to turn your speakers on.
For Healthcare Professionals
In addition to improved patient treatment and outcomes research, another focus of the Service is creating continuing education programs for the broader medical community about properly recognizing hip conditions and understanding when specialized care is needed.
Continuing Education
The Professional Education Department provides information to health care professionals through a variety of medical education programs, including continuing medical education lecture series, conferences and symposiums. The department is dedicated to providing timely educational resources to primary care physicians, sub-specialists, managed care groups, primary care hospitals and associated health professionals. The department also provides a mix of state-of-the-art live programs in addition to online program offerings, monographs, hands-on, skill-based sessions, and didactic lectures. HSS offers a range of on-site professional and continuing medical education programs related to hip pain, preservation, and treatment.
Hip Preservation Fellowship
The goal of the Hip Preservation Fellowship is to offer the fellow clinical experience in the recognition and management of hip pain in the young, active adult hip. In addition to providing clinical opportunities in outpatient settings, the program is also designed so that the fellow will have an active and broad surgical experience, including arthroscopic procedures of the hip, complex hip and pelvis osteotomies, and open surgical dislocations of the hip. The fellow will also interact with other members of the care team, including radiologists, physiatrists, physical therapists, and researchers. This multidisciplinary approach allows the fellow to broaden his or her knowledge base in a wide range of hip conditions and their respective treatment protocols.
How to Make a Referral
You or your patient can call the Hip Preservation Service by telephone weekdays between 9am and 5pm ET at 800.796.0473. On evenings and weekends, leave a voice message and we will return your call.
HSS Connect will answer any questions you may have.
Research
Our Service researchers are establishing a clinical database to evaluate diagnosis and treatment options that will benefit our patients as well as the outside world. Researchers are focusing on new ways and techniques to treat hip pain. One of the goals of the Service's research will be to learn if hip arthroscopy will change the course of arthritis. Research will look deeper into the underlying causes of osteoarthritis of the hip through imaging and biomechanical studies and focus on new surgical techniques and hip preserving procedures.
Clinical Trial: To Understand the Reason for Motion Limitations in Patients with FAI
The Motion and Muscle Analysis in Individuals with Femoral Acetabular Impingement: A Pilot Study
Femoroacetabular Impingement (FAI) occurs when the ball (head of the femur) does not have full range of motion in the socket (acetabulum of the pelvis) due to excess bone. The resulting friction in the hip joint can cause damage to the soft tissue that lines the socket. People with FAI experience pain during common daily activities such as sitting, stair climbing, and even walking. It is currently unclear how the abnormal bone and soft tissue injury affect the muscles around the hip, and why this causes a change in walking patterns and movement.
The Motion and Muscle Analysis in Individuals with Femoral Acetabular Impingement: A Pilot Study will help to better understand how selected hip muscles contribute to different motions. Subjects enrolled in the study, including people with FAI and people with normal anatomy are tested at the Leon Root, M.D Motion Analysis Lab. Reflective markers and electrodes are attached to the body so motion can be recorded on video and electrical activity from muscles can be measured during walking, stair climbing, and other exercise type activities.
Understanding the reason for motion limitations in patients with FAI will help to develop more effective nonsurgical treatments and postoperative rehabilitation plans.
This research study was recruiting both healthy male volunteers age 18-46 and males age 18-45 who were diagnosed with FAI.
Registry
Our registry will enable our clinicians to analyze clinical, radiographic and imaging data on patients to document outcomes for two, five, ten and twenty years following treatment. The registry will help investigators learn which patients make the best candidates for hip arthroscopy and will aid in the development of optimal standards of care and treatment, as well as offer non-operative solutions.
Why choose HSS? Our patients say it best.
In the News
- What Exactly Does Hip Dysplasia Mean for Babies?
- WWE Undertaker documentary: Review of second episode, ‘The Redemption’
- 10 things to know about Hospital for Special Surgery for 2020
- HSS names pair of specialty chiefs — 5 insights
- HSS Names Steve Lee, MD, new Chief of Hand, and Ernest Sink, MD, new Chief of Hip Preservation
- Winning Tennis Titles Again, Bob Bryan Is Inspiring Athletes With Hip Injuries
- HSS Co-sponsors Orthopaedic Conference in India
- A Surgery That Could Save Andy Murray's Tennis Career
- 'It's not a great place to be': Why Ravens QB Joe Flacco's hip injury is worrisome
- Medical residents can now practice virtual operations before they ever touch a live patient
- Big Show healthy and hoping to return to WWE action in 'next couple of weeks'
- Milagro medico para una joven dominicana: volvio a caminar
- Hospital For Special Surgery llego a Peru para presentar sus mas destacados programas
- Hip Joints: Is Preservation or Replacement the Best Option?