Staged Transfemoral Amputation and Osseointegration Limb Reconstruction for Chronic Periprosthetic Knee Infection in a 47-Year-Old Man
From Grand Rounds from HSS: Management of Complex Cases | Volume 15, Issue 1
Case Report
A 47-year-old man was referred for management of end-stage periprosthetic joint infection (PJI) of the right knee. The knee had undergone 20+ surgeries over 15 years, starting with anterior cruciate ligament reconstruction, followed by total knee arthroplasty that was complicated by patellar tendon rupture and subsequent infection. After 3 failed 2-stage knee revisions he presented with a painful static cement spacer on antibiotic suppression (Figure 1a). His arthroplasty surgeons recommended knee arthrodesis or above-knee amputation. The patient was familiar with knee fusion, given his static spacers, and elected for amputation. He was otherwise healthy and desired a high level of function with an amputation; after discussing the risks and benefits of osseointegration limb reconstruction versus a traditional socket prosthesis, he decided on osseointegration.
Standing radiographs showed periosteal reaction to the distal femoral isthmus, and given the chronicity of his infections the decision was made to stage the transfemoral amputation and osseointegration implant insertion (Figure 1b). During the amputation, the tibial and peroneal nerves underwent targeted muscle reinnervation to the motor branches of the medial and lateral hamstrings, respectively. Cement mixed with tobramycin and vancomycin was placed in the femoral canal, and the remaining musculature was purse stringed around the residual femur. His proximal cultures were negative, and so no further antibiotic treatment was given. Approximately 8 weeks later, the antibiotic spacer was removed and a press fit femoral osseointegration implant was placed in a percutaneous procedure (Figure 2a). Cultures of the canal remained negative.

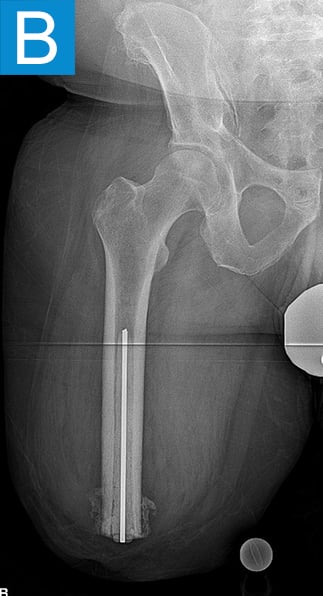
Figure 1. Preoperative X-rays show (A) static cement spacer on antibiotic suppression and (B) an antibiotic cement spacer in the residual femur.
He started progressively loading the implant at 2 weeks and received his full prosthetic leg with simple hinged knee at 6 weeks. At 3 months he no longer used assist devices and at 3.5 months his prosthesis was changed to a microprocessor-controlled knee. Shortly after receiving the new knee, he stumbled stepping over a ledge and fell, sustaining a subtrochanteric proximal femur fracture (Figure 2b). The fracture extended to the tip of the implant, which remained stable in the bone. He underwent open reduction and internal fixation of the femur fracture with a proximal locking plate (Figure 2c). He did not wear the prosthetic leg for 10 weeks, when he began gradually loading the femur. He resumed full weightbearing without assistive devices about 6 weeks later.
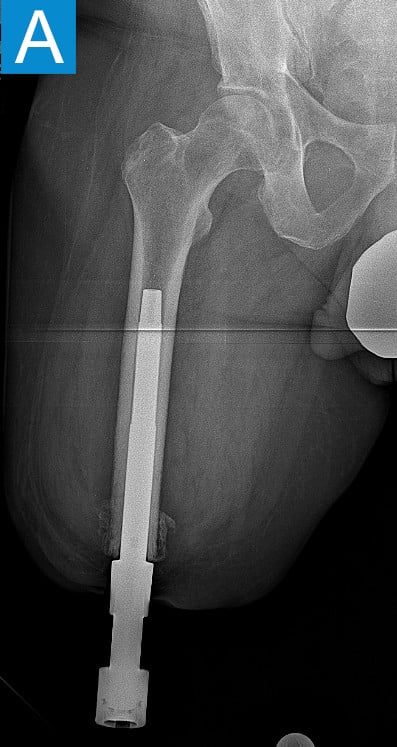

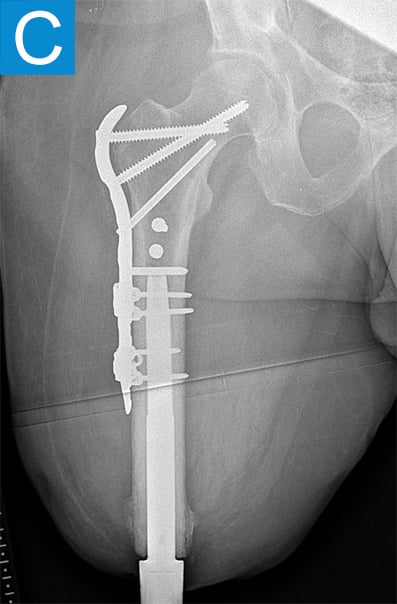
Figure 2. Postoperative X-rays shows (A) a femoral osseointegration implant; (B) a subtrochanteric proximal fracture; (C) the femur fracture repaired by open reduction and internal fixation with a proximal locking plate.
Eighteen months following the osseointegration implant insertion, he noted his medial thigh tissues were progressively sagging, which was causing painful irritation of the skin around the aperture site (Figure 3a). This could not be adequately managed with clothing modifications and external treatments, so he underwent medial thigh excision approximately 2 years after the initial procedure (Figure 3b). Once healed, the pain along the skin portal improved and he resumed unrestricted activity. Three and half years following implant insertion, the patient noted ongoing mild drainage from the skin portal but not enough to require gauze wrapping. Radiographs demonstrated distal medullary bone resorption around the implant, but it was otherwise stable, allowing full activity (Figure 4).


Figure 3. Photographs show (A) skin irritation around the aperture 18 months after the procedure and (B) medial thigh excision 2 years after the initial procedure.
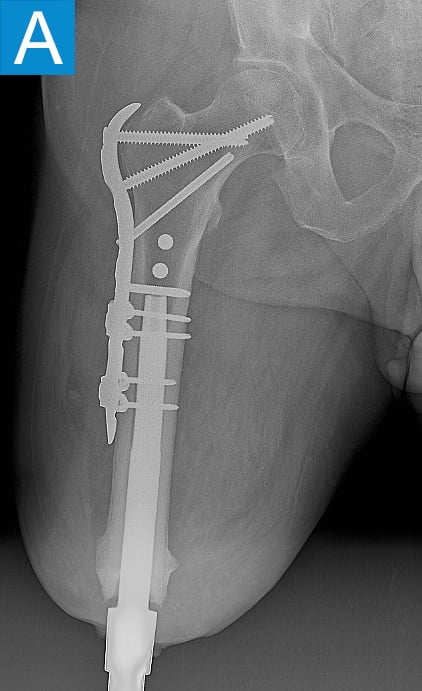

Figure 4. Radiographs 3.5 years after the initial procedure show a stable implant, despite distal medullary bone resorption.
Discussion
Chronic PJI of the knee that has failed to respond to multiple 2-stage revisions usually requires either knee arthrodesis or above-knee amputation. The bone stock for true knee arthrodesis is often deficient, and living with a straight leg is difficult for many people, often necessitating amputation. In healthy patients who want to live independently and be active, socket prosthetics are a challenging long-term solution. Osseointegration limb reconstruction can provide better function and quality of life [1], although it has its own challenges, which this case demonstrates.
Periprosthetic fracture around osseointegrated stems is not surprising, given the stress concentration that occurs proximally to the stem. The incidence is around 5% and mostly due to falls [2]. The stems themselves are nearly always stable in the bone because the osseointegration is robust. This was true in this patient despite less than 4 months of integration time. Thus, the stem can nearly always be maintained and the fracture fixation follows familiar principles. Many periarticular plating options now exist for the femur so that screws can be placed into the diaphysis around the stem to achieve proximal fixation. With stable fixation the healing is usually routine because the forces on the fracture are minimal without the prosthesis attached. Patients usually go back to their prior level of function once healed [2].
Revision of the thigh soft tissues is even more common, with an incidence between 10-30% [3]. New amputees especially have not undergone the usual atrophy of the muscle that occurs with any amputation, so once this happens the subcutaneous tissue begins to sag, which leads to symptoms at the skin portal. Excision of tissue can improve these symptoms [4]. In general, an aggressive excision of subcutaneous tissue is indicated any time osseointegration is performed.
Finally, distal bone resorption is commonly seen the longer osseointegration stems are followed. Potentially a combination of stress shielding and low-grade infection, it is usually monitored unless voluminous drainage or pain warrants an intervention. As with this patient, satisfaction with femoral osseointegration is high despite these issues [5].
Authors

References
- Reif TJ, Khabyeh-Hasbani N, Jaime KM, Sheridan GA, Otterburn DM, Rozbruch SR. Early experience with femoral and tibial bone-anchored osseointegration prostheses. JB JS Open Access. 2021;6(3):e21.00072. doi: 10.2106/JBJS.OA.21.00072.
- Hoellwarth JS, Tetsworth K, Kendrew J, et al. Periprosthetic osseointegration fractures are infrequent and management is familiar. Bone Joint J. 2020;102-B(2):162-169. doi: 10.1302/0301-620X.102B2.BJJ-2019-0697.R2.
- Reetz D, Atallah R, Mohamed J, van de Meent H, Frölke JPM, Leijendekkers R. Safety and performance of bone-anchored prostheses in persons with a transfemoral amputation: a 5-year follow-up study. J Bone Joint Surg Am. 2020;102(15):1329-1335. doi: 10.2106/JBJS.19.01169.
- Vaeth AM, Black GG, Qin N, Et al. The role of concurrent thigh lifts in obese patients with transfemoral osseointegrated prostheses. Ann Plast Surg. 2025;94(4S Suppl 2):S256-S259. doi: 10.1097/SAP.0000000000004286.
- Handford C, McMenemy L, Kendrew J, et al. Improving outcomes for amputees: The health-related quality of life and cost utility analysis of osseointegration prosthetics in transfemoral amputees. Injury. 2022;53(12):4114-4122. doi: 10.1016/j.injury.2022.10.007.