Reconstruction of Complex Flatfoot Deformity with a Dorsal Bunion
From Grand Rounds from HSS: Management of Complex Cases | Volume 8, Issue 2
Case Report
A 27-year-old man was evaluated in March 2016 for left foot pain in the setting of severe left flatfoot deformity and a dorsal bunion (Fig. 1). He stated that his foot had been deformed since a sledding accident at 4 years of age; he had been placed in a long leg cast after a femur injury, but no foot injury had ever been noted.


Figure 1: Weight-bearing radiographs at initial presentation showed significant flatfoot deformity, including (A) anteroposterior view with significant talar head uncovering and talonavicular joint arthritis and (B) lateral view showing a plantarflexed talus with an apex plantar midfoot deformity and an elevated first ray.
The patient’s pain was noted primarily at the sinus tarsi and along the medial arch. His past medical history included congenital pulmonary stenosis and growth delay requiring growth hormone supplementation. He previously smoked half a pack of cigarettes a day, which he stopped in order to decrease his perioperative risk. Initial conservative treatment including shoe lifts and orthotics had not alleviated his foot pain, and although he reported short-term relief with an ultrasound-guided corticosteroid injection into the subtalar joint in June 2016, these conservative measures ultimately failed.
On examination, he had subtle left-hindfoot valgus, pain at the sinus tarsi with forefoot supination, and an elevated first ray with a very prominent dorsal bunion and flexion contracture at the first metatarsophalangeal joint. He had overpull of the anterior tibial tendon, minimal eversion strength/motion, and limited inversion strength/motion. A weight-bearing computed tomographic (CT) scan showed talocalcaneal impingement at the angle of Gissane along with talonavicular arthritis (Fig. 2). There was significant midfoot deformity with shortening of the medial column, a 45° plantarflexion deformity of the talus, and a 45° dorsiflexion deformity through the naviculocuneiform joint in the sagittal plane with elevation of the first and second metatarsals. Talar head uncoverage was noted at the talonavicular joint with flattening of the talar head. A bony irregularity at the anterior aspect of the talocalcaneal joint—a superior projection of the distal aspect of the talus known as talar beaking—suggested a nonosseous coalition.
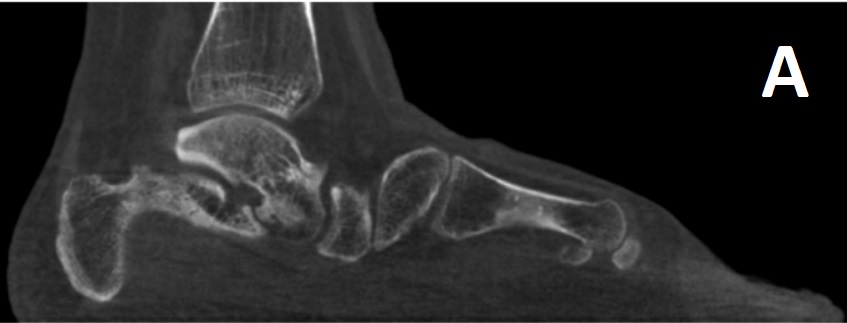


Figure 2: Preoperative weightbearing CT scan showed (A) sagittal view with marked plantar sagging of the head of the talus and navicular with elevation of the first ray at the naviculocuneiform joint, (B) sagittal view with a subtalar non-osseous coalition with talar beaking, and (C) coronal view with lateral impingement.
Surgery was performed in April 2018. The subtalar joint was prepared and realigned through a sinus tarsi approach and fused with two partially threaded cannulated screws. The dorsal bunion was corrected through realignment arthrodesis of the naviculocuneiform and talonavicular joints. The navicular was translated medially and plantarly to correct forefoot abduction and dorsal translation. An 8-mm dorsal wedge was placed from the medial approach into the naviculocuneiform joint (apex plantar). This was fixed with three cannulated compression screws and two locked compression plates (Fig. 3). The tibialis anterior was transferred with maximal length from the first ray to the lateral cuneiform, which reduced the deforming force on the first metatarsal yet maintained ankle dorsiflexion. The extensor hallucis longus was lengthened to allow great toe flexion. The forefoot was then plantigrade and well aligned (Fig. 3).



Figure 3: Radiographs at 1 year postoperatively showed healed (A) subtalar and (B) midfoot fusions and (C) improved hindfoot alignment.
Postoperatively, the patient was placed in a short leg splint, which was changed to a short leg cast at 2 weeks and a controlled ankle movement boot at 7 weeks. At 12 weeks a CT scan showed well-maintained alignment and hardware placement, with good bony ingrowth at the dorsal wedge and fusion sites, and the patient began partial weight bearing. At 6 months he progressed to wearing regular shoes and had no pain. At 1 year he could work full time and occasionally run and play basketball, all pain free. Examination showed neutral hindfoot alignment, correction of forefoot abduction, and markedly improved first ray alignment (Fig. 4).
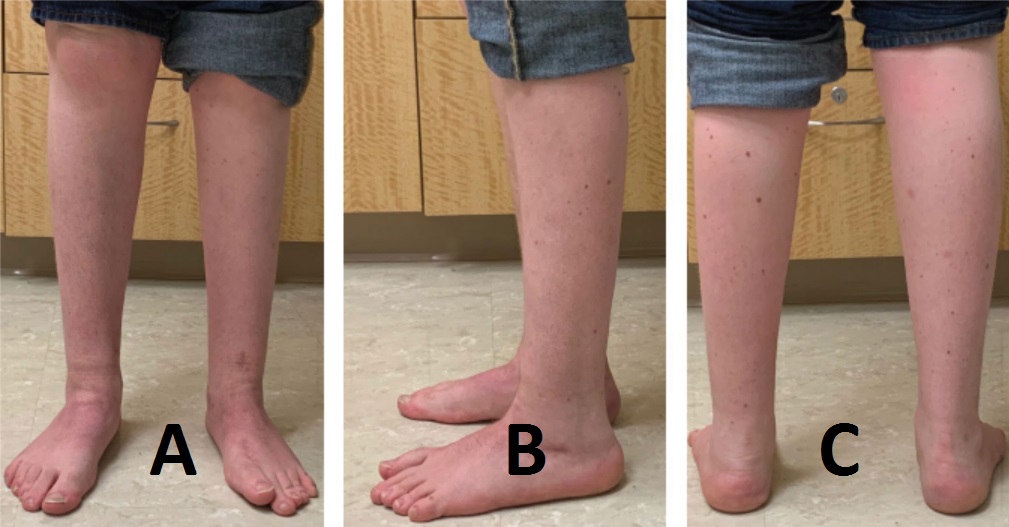
Figure 4: : Postoperative (A) anterior, (B) lateral, and (C) hindfoot alignment clinical views at 1 year showed improved midfoot, first ray, and hindfoot alignment of the left foot.
Discussion
This complex case of flatfoot deformity with a dorsal bunion was managed with subtalar, talonavicular, and naviculocuneiform fusions; tibialis anterior transfer; and extensor hallucis longus lengthening.
The dorsal bunion was first described by Lapidus in 1940 as a dorsiflexion deformity of the first ray associated with flexion of the great toe at the first metatarsophalangeal joint [2]. Dorsal bunion deformity is rare, with reports in the literature limited to case series, usually in children [3]. It is most often seen after operative correction of clubfoot deformity, but other causes include paralytic foot conditions and severe congenital flatfoot [1, 2]. Although our patient reported no history of congenital foot disorders, he may have had a congenital flatfoot or coalition that remained subclinical until his childhood trauma. He may also have experienced a post-traumatic flatfoot deformity [4].
To correct the dorsal bunion, we performed a plantarflexion arthrodesis of the naviculocuneiform joint with interposition of a dorsal wedge and a talonavicular fusion [1]. Transfer of the tibialis anterior also permitted rebalancing of the deforming force of dorsiflexion [1]. This reconstruction has been described, involving the addition of a second tricortical allograft bone-block wedge into the first and second intercuneiform joints, which produced good outcomes [1].
This case also highlights the utility of weightbearing CT scan (Fig. 2), now routinely available at our institution and elsewhere. The images indicated the need for a subtalar fusion based on the lateral impingement identified and also allowed for preoperative planning specific to wedge grafting of the naviculocuneiform fusion
Posted: 7/1/2019
Authors
Aoife MacMahon, BA
MD Candidate, Class of 2020
Weill Cornell Medicine
Lauren E. Roberts, MD, MSc, FRCSC
Attending Orthopaedic Surgeon
University of British Columbia, Vancouver,
British Columbia, Canada
Orthopaedic Surgery Clinical Fellow
Class of 2018
Hospital for Special Surgery

Attending, Orthopedic Surgery, Hospital for Special Surgery
Professor of Orthopedic Surgery, Weill Cornell Medical College
References
- Johnson JE, Thomson AB, Yu JR. Double bone-block arthrodesis for the correction of a dorsal bunion deformity. Tech Foot Ankle Surg. 2007;6(3):170–174.
- Lapidus PW. “Dorsal bunion”: its mechanics and operative correction. J Bone Joint Surg Am. 1940;22(3):627–637.
- McKay D. Dorsal bunions in children. J Bone Joint Surg Am. 1983;65(7):975–980.
- Nelson DR, Younger A. Acute posttraumatic planovalgus foot deformity involving hindfoot ligamentous pathology. Foot Ankle Clin. 2003;8(3):521–537.