Osteomyelitis Requiring Open Debridement After Intertrochanteric Femur Fracture in a 62-Year-Old Man
From Grand Rounds from HSS: Management of Complex Cases | Volume 12, Issue 1
Case Report
A 62-year-old man sustained a ground-level fall resulting in a right intertrochanteric femur fracture in June 2020. He was overweight (body mass index of 26.55) and his prior medical history included asthma requiring intubation, hypertension, type 2 diabetes, vertebral osteomyelitis/epidural abscess, and pulmonary embolus. He underwent operative fixation at another hospital shortly after injury (Fig. 1). His postoperative course was complicated by infection requiring operative debridement 2 months later. On postoperative day 1, against medical advice, the patient sought evaluation at another hospital. He was ultimately discharged from that hospital and had follow-up with the primary surgeon.
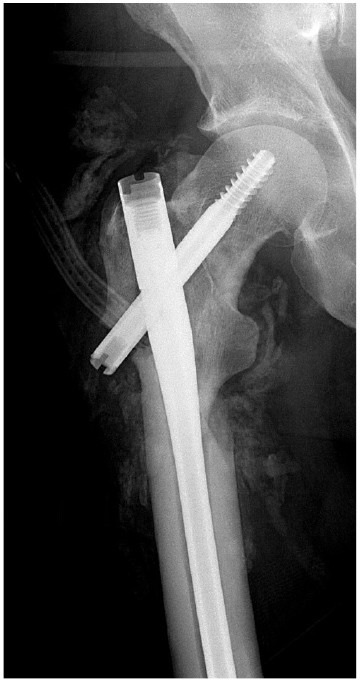
Figure 1: Plain X-ray of the right hip, the first taken after initial debridement.
For the next year, the patient completed multiple rounds of antibiotics and underwent several more surgeries. In July 2021, he presented to the emergency department (ED) with persistent complaints of pain in the right hip and a sinus of draining purulence. Computed tomography (CT) revealed a right intertrochanteric fracture nonunion with well-circumscribed fluid collection (Fig. 2); the patient underwent open debridement, hardware removal, fracture stabilization, and antibiotic bead placement (Fig. 3). Deep cultures taken at this time revealed no bacterial growth. Of note, the patient had been maintained on dual antibiotic therapy for 8 weeks prior. Postoperatively, he was maintained on antibiotics and observed clinically and was discharged after 5 days.

Figure 2: X-rays of the right hip at presentation; the patient had erythema and drainage from the previous surgical incision.

Figure 3: X-rays after removal of the intramedullary nail show antibiotic beads and fracture fixation.
The patient returned 3 weeks later with persistent pain and swelling in the right thigh. A CT scan revealed a large fluid collection, and again the patient returned to the operating room for serial debridement and placement of non-biodegradable antibiotic beads. He was discharged 9 days after the last of 3 debridement procedures.
Serial X-rays showed continued fracture healing until March 2022, when the patient returned to the ED with swelling and erythema. A CT scan showed a fluid collection and a healed fracture (Figs. 4, 5), at which point he underwent repeat debridement and hardware removal.
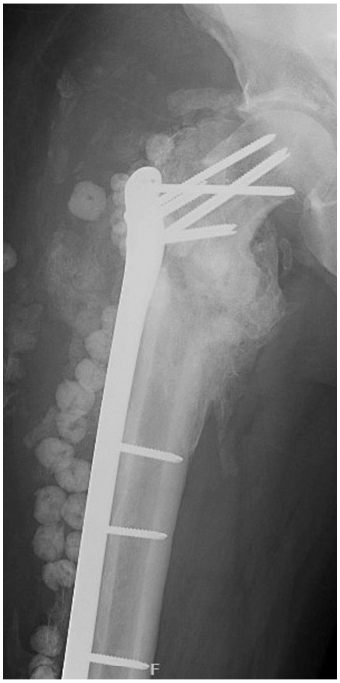
Figure 4: X-rays reveal interval healing of the right hip.
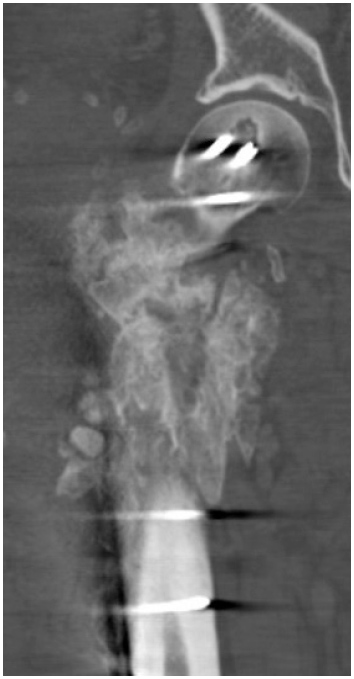
Figure 5: A CT scan reveals fluid collection and interval fracture healing.
Postoperatively, he slowly returned to function and showed no further evidence of infection (Fig. 6). At the most recent follow-up in September 2022, the patient was ambulating with a cane and actively engaging in physical therapy.

Figure 6: Final X-rays reveal healed right proximal femur.
Discussion
Postoperative infection after hip fracture surgery occurs in 2.1% patients and in 1.35% of patients undergoing fixation, resulting in extensive treatments and costs [1]. Our patient’s late infection developed into osteomyelitis, which is very challenging to eradicate [2]. Our treatment goals were to suppress infection and encourage fracture healing [3]. A healed fracture allows for hardware removal, which eliminates plate and screws from the infection equation. Another option would have been to remove hardware earlier and treat the infection with debridement and antibiotics; given the instability of the fracture and the location, this was a less favorable option.
A patient’s return to function in the immediate postoperative period is vital to recovery [4], although mobilization and weightbearing after hip fracture can be difficult. This case illustrates that, although the patient’s clinical course evolved over 2 years, fracture union and decreased bacterial burden to a subclinical level were achieved [5].
References
- Masters J, Metcalfe D, Ha JS, Judge A, Costa ML. Surgical site infection after hip fracture surgery: a systematic review and meta-analysis of studies published in the UK. Bone Joint Res. 2020;9(9):554-562. doi: 10.1302/2046-3758.99.BJR-2020-0023.R1.
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364(9431):369-79. doi: 10.1016/S0140-6736(04)16727-5.
- Gardner MJ, Toro-Arbelaez JB, Harrison M, Hierholzer C, Lorich DG, Helfet DL. Open reduction and internal fixation of distal femoral nonunions: long-term functional outcomes following a treatment protocol. J Trauma. 2008;64(2):434-8. doi: 10.1097/01.ta.0000245974.46709.2e.
- Loggers SAI, Van Lieshout EMM, Joosse P, Verhofstad MHJ, Willems HC. Prognosis of nonoperative treatment in elderly patients with a hip fracture: A systematic review and meta-analysis. Injury. 2020;51(11):2407-2413. doi: 10.1016/j.injury.2020.08.027.
- Lam A, Richardson SS, Buksbaum J, Markowitz J, Henry MW, Miller AO, Rozbruch SR, Fragomen AT. Chronic osteomyelitis of the tibia and ankle treated with limb salvage reconstruction. J Bone Jt Infect. 2019;4(6):306-313. doi: 10.7150/jbji.40337.