Hypertrophic Tibial Nonunion Treated with AutoStrut External Fixation
From Grand Rounds from HSS: Management of Complex Cases | Volume 11, Issue 2
Case Report
A 57-year-old man presented with a previously infected, distal tibial hypertrophic nonunion with associated deformity. He had sustained a closed fracture after a skiing accident that was initially treated with a plate and screws. His clinical course was complicated by wound breakdown and osteomyelitis necessitating hardware removal, a medially based free flap, and 6 weeks of IV antibiotics. His peroneal artery was injured and his posterior tibial artery was sacrificed for the free tissue transfer, leaving him with an anterior tibial artery. Now unstable, his distal tibial fracture was placed into an ankle foot orthosis, which did not prevent progressive tibial deformity. At the time of initial consultation, he had been off antibiotics for 2 months without signs of infection and had pain with ambulation, varus deformity, shortening, and external rotation of the foot. His skin was closed with woody swelling. The nonunion had less than 5° of motion on stress examination.
Preoperatively, the patient was noted to have a distal tibial hypertrophic nonunion; an intact fibula; varus 15°; apex anterior 4°; distal tibial external rotation 10° and 15 mm shortening; a history of osteomyelitis without clinical signs of infection; and a free tissue transfer with a single vessel limb (Fig. 1 & 2). Fibular osteotomy was required to allow repositioning of the tibia. We assessed the mobility of the hypertrophic tibial nonunion after fibular osteotomy and confirmed it was not consolidated. We used a percutaneous anterior approach to reach the nonunion site, from which we took tissue samples to test for suspected fracture-related infection [1]. The mobility was less than 10°, and it was decided that the fibrous tissue had enough stiffness to allow for distraction, in that it would have the capacity to mineralize under tension. A hexapod frame with automatic struts (AutoStrut, OrthoSpin) was applied for gradual correction of the multiplanar deformity. The rings were stabilized with strong fixation to ensure adequate power to pull through the stiff nonunion tissue. The rings were connected with automatic struts with their own motors, battery, and computer system. An adjustment schedule was created and uploaded into the head unit of the frame’s computer.

Figure 1: Clinical photograph shows a deformed leg with a medial free tissue transfer flap and chronic lymphedema.

Figure 2: Radiographs show a hypertrophic nonunion of the distal tibia with shortening and deformity in both the coronal (A) and sagittal (B) planes.
The schedule started Day 1 postoperatively and was broken into 8 movements each day per strut (Fig. 3). Intraoperative tissue cultures were negative for infection. After 40 days of correction, a residual schedule was used to apply oblique compression across the nonunion site to enhance healing after evaluation with computed tomography. Iliac crest bone graft was applied to the nonunion site 6 months after frame application to augment the partial healing attained with distraction. The foot ring was removed at the same setting to allow for ankle mobility. The frame was removed 10 months after application. Now, 16 months after frame removal, the patient is infection free, works full time, and cycles aggressively, all without pain or medication (Fig. 4 & 5).
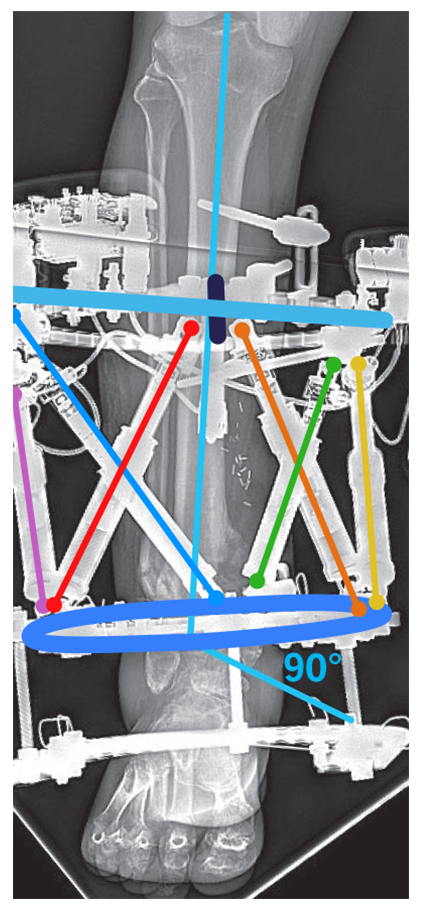
Figure 3: The motorized and computerized external fixator is shown mid-correction. The foot ring was used temporarily to prevent ankle contracture.
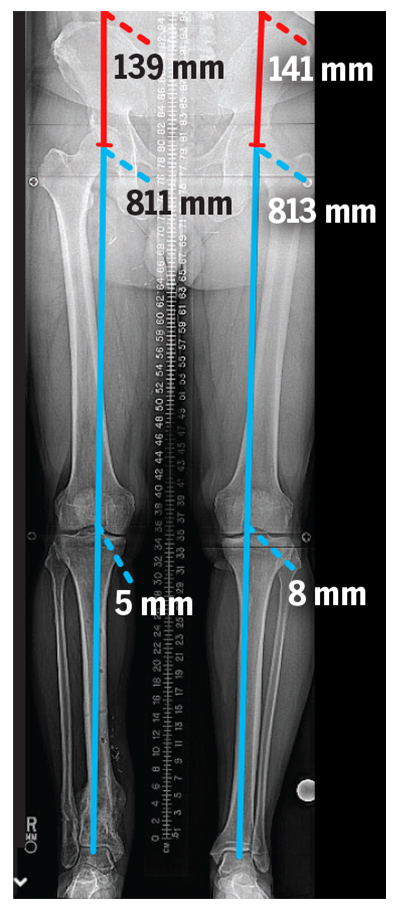
Figure 4: The final standing X-ray shows re-establishment of leg length and a normal mechanical axis.

Figure 5: A lateral X-ray shows distal tibial union after treatment, with a successful realignment.
Discussion
Stiff, hypertrophic nonunions can be treated with distraction osteogenesis by pulling traction slowly through the nonunion site [2]. The fibrocartilaginous nonunion tissue has regenerative potential in a stable mechanical environment. While most commercially available hexapod, circular external fixators have been witnessed performing this amazing biological feat, the automatic adjusting struts remain untested.
This case highlights the AutoStrut’s ability to pull through a stiff nonunion with power and accuracy. This patient’s deformity and nonunion were managed simultaneously with a hexapod frame. The AutoStrut has been shown to work well after osteotomy [3]; the struts were programmed to allow hands-free adjustment for pain reduction and patient convenience and were strong enough to move the bone fragments into the desired position. None of the struts misbehaved and no numbers shifted after completion of the program.
Authors

Attending Orthopedic Surgeon, Hospital for Special Surgery
Director, Limb Salvage and Amputation Reconstruction Center, Hospital for Special Surgery
Steven J. Wallace, MD
Post-Fellowship Contributor
Limb Lengthening and Complex Reconstruction
References
- Govaert GAM, Kuehl R, Atkins BL, et al; Fracture-Related Infection (FRI) Consensus Group. Diagnosing fracture-related infection: current concepts and recommendations. J Orthop Trauma. 2020;34(1):8-17. doi: 10.1097/BOT.0000000000001614.
- Rozbruch SR, Fragomen AT, Ilizarov S. Correction of tibial deformity with use of the Ilizarov-Taylor spatial frame. J Bone Joint Surg Am. 2006;88 Suppl 4:156-174. doi: 10.2106/JBJS.F.00745.
- Geffner AD, Reif TJ, Fragomen AT, Rozbruch SR. Use of Orthospin technology in the correction of complex limb deformities. Annals of Robotics and Automation. 2021;5(1):37-40.