Chronic Hip Periprosthetic Joint Infection Requiring Revision Through an Approach that Differed from the Index Arthroplasty
From Grand Rounds from HSS: Management of Complex Cases | Volume 13, Issue 1
Case Report
A 57-year-old man presented with an infected left total hip arthroplasty (THA). He had undergone elective left THA at an outside institution through a direct anterior approach; 2 weeks after surgery, he noticed incisional swelling and drainage, and at 6 weeks and 9 weeks he underwent irrigation and debridement. A subsequent hip aspiration was positive for Staphylococcus epidermidis, and he was placed on oral antibiotics. At 3 months he sought a second opinion at HSS.
On examination, the patient was found to have persistent drainage and cutaneous pustules around his anterior incision and 2 draining sinuses. He had a body mass index of 28.5 and was febrile. Range of motion included 90° of flexion and 30° of external rotation, limited by pain. Due to his components being well fixed (Fig. 1), the patient agreed to undergo an extensile posterior approach to the hip.
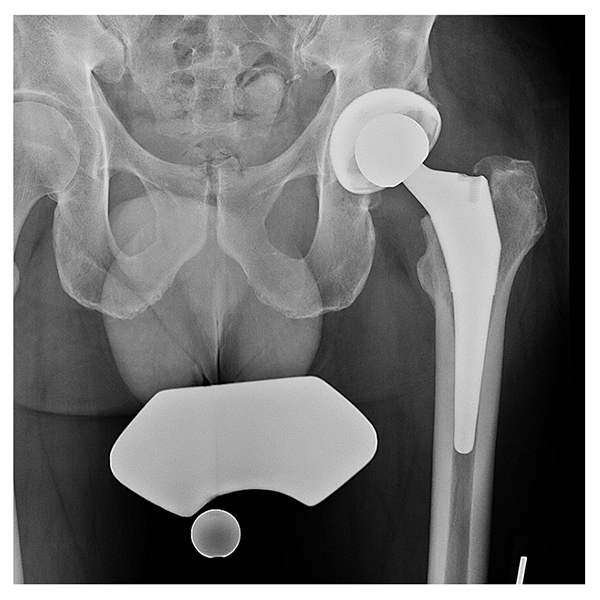
Figure 1: Preoperative radiograph demonstrating a cementless THA with well-fixed components.
The components were safely removed without a trochanteric osteotomy. The anterior incision was included within the sterile field so that it could be debrided, and the anterior interval was identified from the posterior approach. Scrub brushes with 10% povidone iodine were used to debride the posterior and anterior tracts and the bony surface; the wound was irrigated and immersed in 10% povidone iodine for 10 minutes, and an articulating spacer with antibiotic cement (high-viscosity Palacos [R+G] cement containing gentamicin 0.5 g and vancomycin 2 g) was placed (Fig. 2).

Figure 2: Postoperative radiograph demonstrating an articulating hip spacer with a semi-constrained acetabular component and femoral component made intraoperatively from a mold.
Although intraoperative cultures were negative, because of his history of positive intra-articular cultures for S. epidermidis and Escherichia coli, the patient received 6 weeks of IV vancomycin and cefepime. At the 6-week mark, both anterior and posterior incisions had healed, and the patient was compliant with 50% weight-bearing. When after a 2-week antibiotic holiday subsequent blood work and aspiration showed that the infection had resolved, the patient underwent reimplantation through the posterior approach with a revision acetabular component fixed with multiple screws and a diaphyseal engaging modular tapered stem (Fig. 3). It was noted that the anterior wall was deficient due to the underlying infection and explantation procedure. Intraoperative cultures were negative and postoperatively the patient was placed on a progressive weight-bearing routine with posterior precautions.
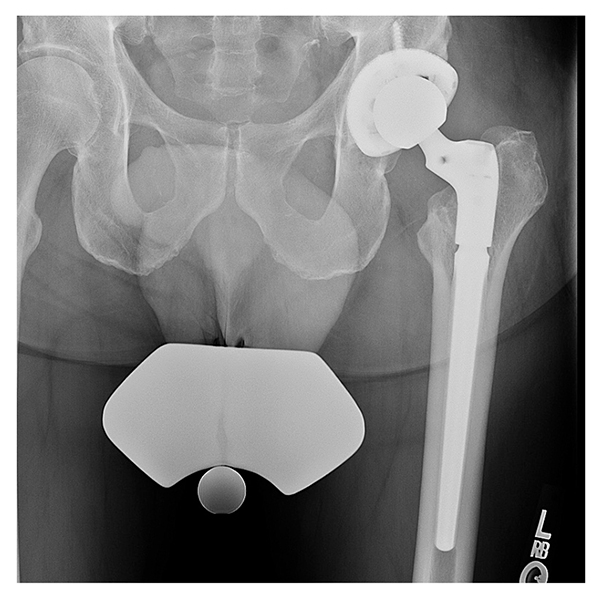
Figure 3: Postoperative radiograph demonstrating cementless revision involving a multihole acetabular cup with multiple screws and a modular tapered diaphyseal engaging stem.
The patient completed postoperative physical therapy and at 13-months post-reimplantation, he remained infection free. He reported episodes of pain associated with iliopsoas tendonitis secondary to anterior wall bone loss that improved with physical therapy, as well as numbness around his anterior incision and along the lateral portion of the thigh that did not affect walking.
Discussion
Management of chronic PJI in patients who have undergone THA through a traditionally non-extensile exposure such as the direct anterior approach poses an interesting challenge to the revision surgeon. Although the direct lateral and posterior lateral approaches provide extensile views of the hip that facilitate component removal, the use of multiple approaches may disrupt muscles critical to hip stability (including the abductors in the direct lateral approach and the short external rotators in the posterolateral approach). These concerns are weighed against the prospect of wound complications in revision through the direct anterior approach [1] that may require release of the posterior fibers to permit adequate femoral elevation [2].
This case illustrates an explantation and reimplantation through the posterior approach without postoperative instability. A lip liner or dual mobility liner may be used at the time of reimplantation in patients with multiple surgical approaches to reduce the risk of instability. Clinical outcomes for patients who have undergone revision through a different approach from the index arthroplasty are not well understood, with only 1 retrospective analysis, a small case series, demonstrating no difference [3]. Thus, the debate over the ideal surgical approach for primary THA continues. The use of high concentration povidone iodine has shown effectiveness against mature staphylococcal biofilm [4] and should be considered when treating acute or chronic PJI.
Authors

Attending Orthopedic Surgeon, Hospital for Special Surgery
Associate Professor, Weill Cornell Medical College
References
- Kurkis GM, Chihab S, Farley KX, Anastasio AT, Bradbury TL, Guild GN. Anterior revision hip arthroplasty is associated with higher wound complications but fewer dislocations compared to posterior revision hip surgery. J Arthroplasty. 2021;36(1):250-254.
- Thaler M, Corten K, Nogler M, Holzapfel BM, Moskal J. Femoral revision with the direct anterior approach. Oper Orthop Traumatol. 2022;34(3):189-202.
- Harmer JR, Wyles CC, Larson DR, Taunton MJ, Pagnano MW, Abdel MP. Changing surgical approach from primary to revision total hip arthroplasty is not associated with increased risk of dislocation or re-revisions. J Arthroplasty. 2022;37(7S):S622-S627.
- Premkumar A, Nishtala SN, Nguyen JT, Bostrom MPG, Carli AV. The AAHKS Best Podium Presentation Research Award: Comparing the efficacy of irrigation solutions on staphylococcal biofilm formed on arthroplasty surfaces. J Arthroplasty. 2021;36(7S):S26-S32.