Chronic Extensor Mechanism Deficiency After Total Knee Arthroplasty: Treatment With Allograft Reconstruction
From Grand Rounds from HSS: Management of Complex Cases | Volume 8, Issue 1
Case Report
A 66-year-old man presented to our institution complaining of 2 years of bilateral knee pain. He had previously undergone bilateral total knee arthroplasty (TKA) at another facility. The surgeries had been a success initially, but 7 years later the patient underwent revision of the right TKA for anterior dislodgement of his tibial polyethylene liner and rupture of the patellar tendon (Fig. 1).

Figure 1: Lateral view of the right knee prior to the patient’s initial revision TKA, showing anterior dissociation of the polyethylene liner.
The tibial liner was restored and the patellar tendon repaired and augmented with an Achilles tendon allograft. Postoperatively, he developed an infected hematoma requiring irrigation and debridement. Ultimately, the patellar tendon repair failed. About 1 year later the patient fell, resulting in rupture of the left quadriceps tendon. This was repaired, but it ruptured again 1 month later and required revision left quadriceps tendon repair and augmentation with an Achilles tendon allograft. After this left knee procedure, the patient developed another hematoma and infection.
On presentation to our facility, the patient complained of pain and weakness in both lower extremities and could not actively extend either knee. He occasionally used bilateral hinged knee braces locked in extension for ambulation but was not reliably compliant with these. He required a walker, could walk only short distances, and was unable to reciprocate stairs. Despite these limitations, the patient continued to work as a schoolteacher. He had been off antibiotics for several weeks and had no signs or symptoms of infection.
On examination, he could ambulate with the aid of a walker and exhibited an antalgic gait pattern. There was a palpable deficiency in the left quadriceps tendon. Both knees had moderate effusions, with range of motion from 25° of hyperextension to 120° of flexion; he could extend neither leg against resistance. Radiographs demonstrated well fixed TKAs with patella alta on the left and patella baja on the right. White blood cell count, erythrocyte sedimentation rate, and C-reactive protein levels were within normal limits, and bilateral knee aspirations showed no evidence of prosthetic joint infection.
We decided to approach the case in a staged fashion, and the patient opted to address the right knee first. Given the significant hyperextension of both knees, we opted to revise the TKAs to hinged prostheses with femoral and tibial cemented diaphyseal stems. During exposure, the deficient extensor mechanism was excised from the tibial tubercle to the proximal pole of the patella, leaving the maximum amount of quadriceps tendon to aid in reconstruction. The same procedure was used for both knees.
Once the revision knee implant had been cemented in place, a trough was made in the anterior tibia in the location of the native tibial tubercle. A ledge of bone was left at the proximal aspect of the tibia to improve graft resistance to tension. A fresh frozen allograft extensor mechanism, including the tibial tubercle, patellar tendon, patella, and quadriceps tendon, was used to reconstruct the extensor mechanism. The tibial tubercle bone fragment was contoured to fit in the trough of the native tibia and was impacted into the bone in a press-fit fashion. Two 3.5-mm screws were used to augment the fixation. With the knee in maximal extension, #5 ethibond sutures were placed in Krackow pattern in both the native and allograft quadriceps tendon. With an assistant applying maximal tension, the 2 quadriceps tendons were repaired to each other in a layered fashion (Fig. 2A and 2B).
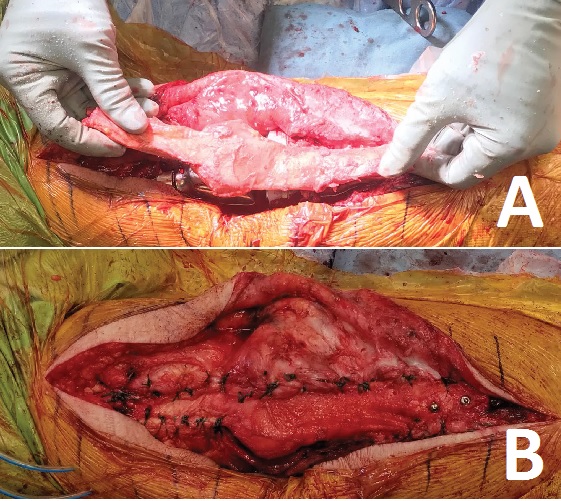
Figure 2: Intraoperative images showing (A) the extensor mechanism allograft overlying the revision total knee replacement and (B) the fully repaired extensor mechanism.
Postoperatively, a clamshell splint in maximal extension was applied until postoperative day 2, when the patient was converted to a cylinder cast. He was allowed to be toe-touch weight bearing while the cast was in place for 8 weeks; he then advanced weight bearing and began structured therapy, with a gradual increase in knee flexion. By 3 months postoperatively, he had no pain and no significant extensor lag and 90° of flexion in both knees (Fig. 3A and 3B).
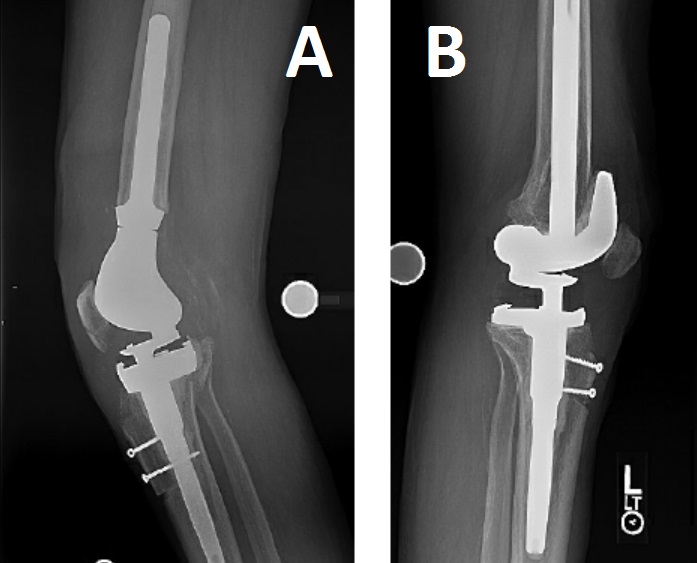
Figure 3: Postoperative lateral images of (A) the right knee and (B) the left knee.
Discussion
Although uncommon, chronic extensor mechanism disruption after TKA is an extremely debilitating complication, as this case demonstrates. Multiple reconstruction techniques have been described in the literature, including the use of an allograft extensor mechanism [2, 4] and a synthetic graft [1, 7]. Appropriate tensioning of the graft and native muscle is critical to avoiding extensor lag; a study comparing minimal to maximal graft tensioning at the time of repair showed an average postoperative extensor lag of 59° in minimally tensioned grafts and 4° in maximally tensioned grafts [3].
When successful, these reconstruction techniques can significantly improve a patient’s function and comfort and overall knee range of motion, as well as reduce extensor lag [1, 4]. A systematic review showed no difference between patient-reported outcome scores, range of motion, or complication rates between reconstructions with allograft or synthetic graft [6].
Despite appropriate technique, patients undergoing extensor mechanism reconstruction are at high risk of postoperative complications. Failure rates have been reported to be as high as 56 to 58% at 10 years, due to a combination of allograft failure, deep infection, persistent extensor lag greater than 30°, and symptomatic graft lengthening [1, 2, 5]. Younger age at the time of reconstruction may predict subsequent graft failure [5].
Posted: 3/1/2019
Authors
Shawn S. Richardson, MD
Orthopaedic Surgery Clinical Fellow
Hospital for Special Surgery

Director, Complex Joint Reconstruction Center
Surgeon-in-Chief Emeritus, Hospital for Special Surgery
References:
- Abdel MP, Salib CG, Mara KC, Pagnano MW, Perry KI, Hanssen AD. Extensor mechanism reconstruction with use of marlex mesh. J Bone Jt Surg. 2018;100(15):1309–1318.
- Brown NM, Murray T, Sporer SM, Wetters N, Berger RA, Della Valle CJ. Extensor mechanism allograft reconstruction for extensor mechanism failure following total knee arthroplasty. J Bone Jt Surg. 2015;97(4):279–283.
- Burnett RSJ, Berger RA, Paprosky WG, Della Valle CJ, Jacobs JJ, Rosenberg AG. Extensor mechanism allograft reconstruction after total knee arthroplasty. A comparison of two techniques. J Bone Joint Surg Am. 2004;86-A(12):2694–2699.
- Lim CT, Amanatullah DF, Huddleston JI, et al. Reconstruction of disrupted extensor mechanism after total knee arthroplasty. J Arthroplasty. 2017;32(10):3134–3140.
- Ricciardi BF, Oi K, Trivellas M, Lee Y, Della Valle AG, Westrich GH. Survivorship of extensor mechanism allograft reconstruction after total knee arthroplasty. J Arthroplasty. 2017;32(1):183–188.
- Shau D, Patton R, Patel S, Ward L, Guild G. Synthetic mesh vs. allograft extensor mechanism reconstruction in total knee arthroplasty. A systematic review of the literature and meta-analysis. Knee. 2018;25(1):2–7.
- Wood TJ, Leighton J, Backstein DJ, et al. Synthetic graft compared with allograft reconstruction for extensor mechanism disruption in total knee arthroplasty. J Am Acad Orthop Surg. October 2018. doi:10.5435/JAAOS-D-18-00393